

Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction
- PMID: 30962192
- PMCID: PMC6662953
- DOI: 10.1136/heartjnl-2018-314173
Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction
Abstract
Background: We assessed the prognostic significance of absolute and percentage change in N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels in patients hospitalised for acute decompensated heart failure with preservedejection fraction (HFpEF) versus heart failure with reduced ejection fraction (HFrEF).
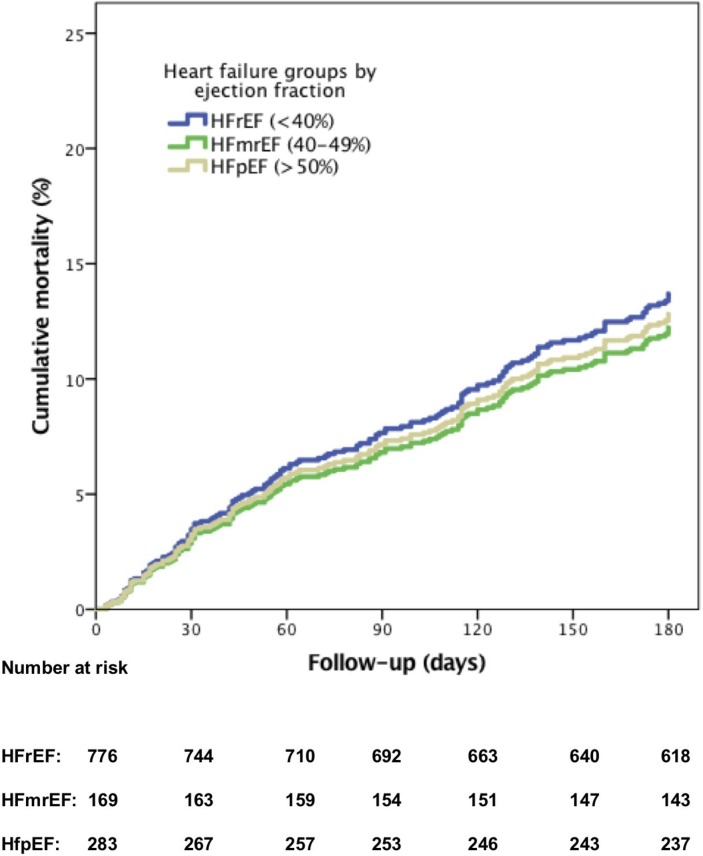
Methods: Patients with left ventricular ejection fraction ≥50% were categorised as HFpEF (n=283), while those with <40% as were categorised as HFrEF (n=776). Prognostic values of absolute and percentage change in NT-proBNP levels for 6 months all-cause mortality after discharge were assessed separately in patients with HFpEF and HFrEF by multivariable adjusted Cox regression analysis. Comorbidities were compared between heart failure groups.
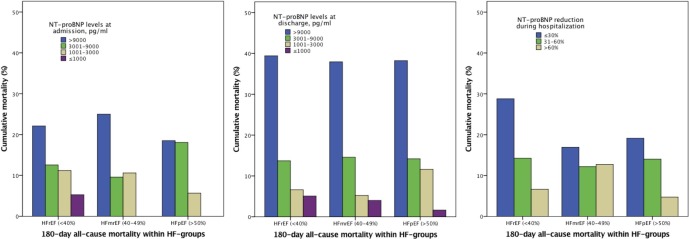
Results: Discharge NT-proBNP levels predicted outcome similarly in HFpEF and HFrEF: for any 2.7-factor increase in NT-proBNP levels, the HR for mortality was 2.14 for HFpEF (95% CI 1.48 to 3.09) and 1.96 for HFrEF (95% CI 1.60 to 2.40). Mortality prediction was equally possible for NT-proBNP reduction of ≤30% (HR 4.60, 95% CI 1.47 to 14.40 and HR 3.36, 95% CI 1.93 to 5.85 for HFpEF and HFrEF, respectively) and for >30%-60% (HR 3.28, 95% CI 1.07 to 10.12 and HR 1.79, 95% CI 0.99 to 3.26, respectively), compared with mortality in the reference groups of >60% reductions in NT-proBNP levels. Prognostically relevant comorbidities were more often present in patients with HFpEF than patients with HFrEF in low (≤3000 pg/mL) but not in high (>3000 pg/mL) NT-proBNP discharge categories.
Conclusions: Our study highlights-after demonstrating that NT-proBNP levels confer the same relative risk information in HFpEF as in HFrEF-the possibility that comorbidities contribute relatively more to prognosis in patients with HFpEF with lower NT-proBNP levels than in patients with HFrEF.
Keywords: NT-proBNP; acute decompensated Heart failure; preserved left ventricle ejection fraction; prognosis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: YMP is a recipient of payments for lectures including service on speakers’ bureaus and research grants from Roche Diagnostics. YMP has an unrelated biomarker patent and stocks in a university spinoff company. WEK received a grant (2010B97) from the Dutch Heart Foundation for the PRIMA II study and has participated in advisory board meetings of Roche Diagnostics and Novartis. MM is a member of the board in Corthera and Novartis and receives payment for lectures including service on speakers’ bureaus from Servier or Stroder.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials