Melatonin as a master regulator of cell death and inflammation: molecular mechanisms and clinical implications for newborn care
- PMID: 30962427
- PMCID: PMC6453953
- DOI: 10.1038/s41419-019-1556-7
Melatonin as a master regulator of cell death and inflammation: molecular mechanisms and clinical implications for newborn care
Abstract
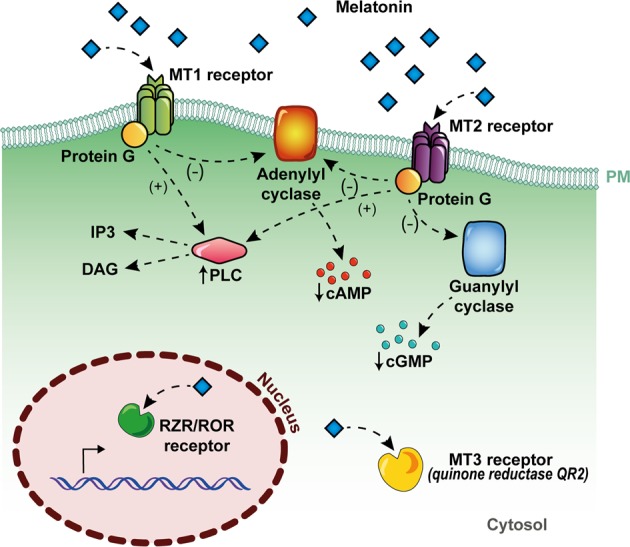
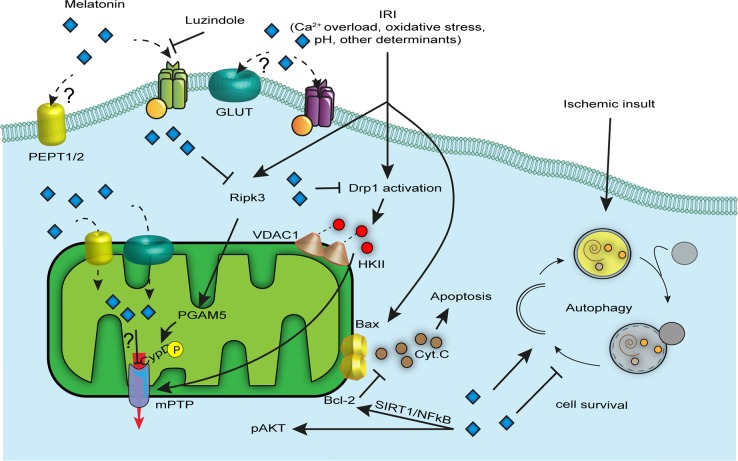
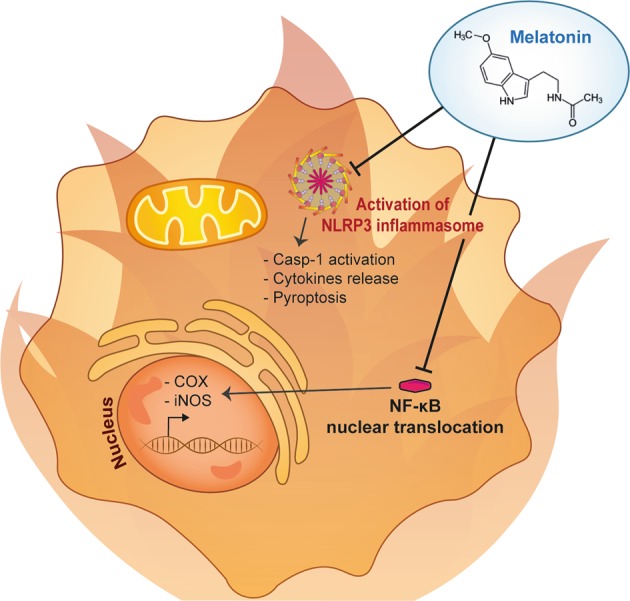
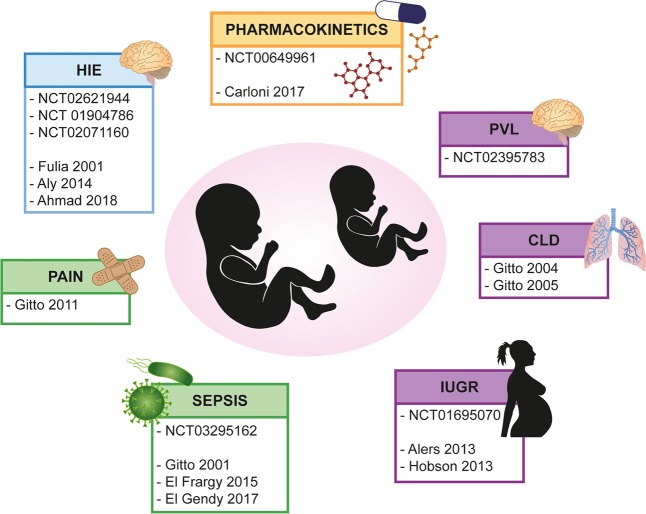
Melatonin, more commonly known as the sleep hormone, is mainly secreted by the pineal gland in dark conditions and regulates the circadian rhythm of the organism. Its intrinsic properties, including high cell permeability, the ability to easily cross both the blood-brain and placenta barriers, and its role as an endogenous reservoir of free radical scavengers (with indirect extra activities), confer it beneficial uses as an adjuvant in the biomedical field. Melatonin can exert its effects by acting through specific cellular receptors on the plasma membrane, similar to other hormones, or through receptor-independent mechanisms that involve complex molecular cross talk with other players. There is increasing evidence regarding the extraordinary beneficial effects of melatonin, also via exogenous administration. Here, we summarize molecular pathways in which melatonin is considered a master regulator, with attention to cell death and inflammation mechanisms from basic, translational and clinical points of view in the context of newborn care.
Conflict of interest statement
The authors declare no competing interests.
Figures