

Transcriptome networks identify mechanisms of viral and nonviral asthma exacerbations in children
- PMID: 30962590
- PMCID: PMC6472965
- DOI: 10.1038/s41590-019-0347-8
Transcriptome networks identify mechanisms of viral and nonviral asthma exacerbations in children
Abstract
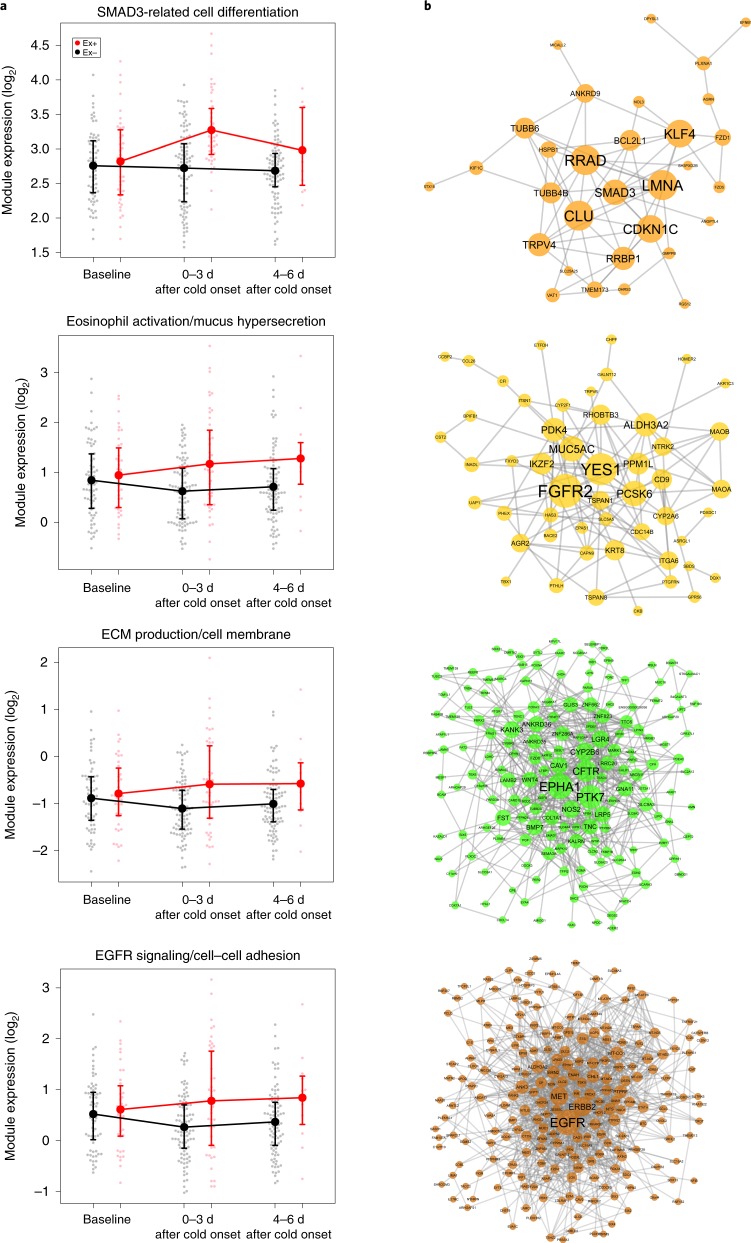
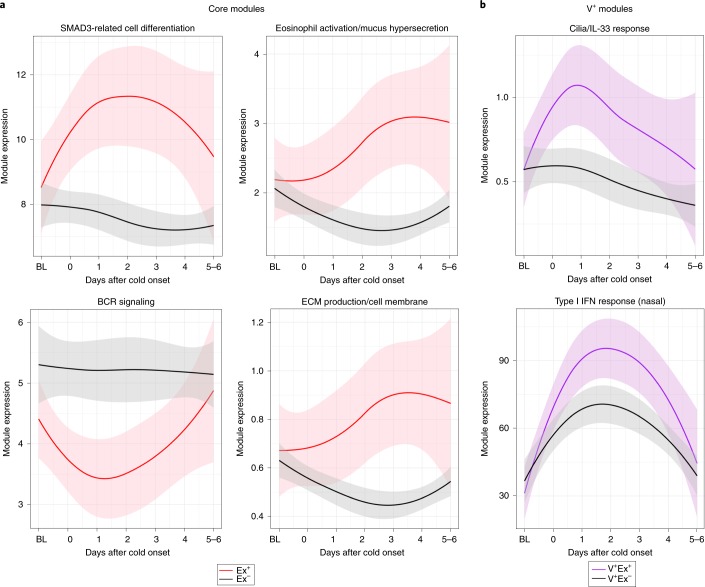
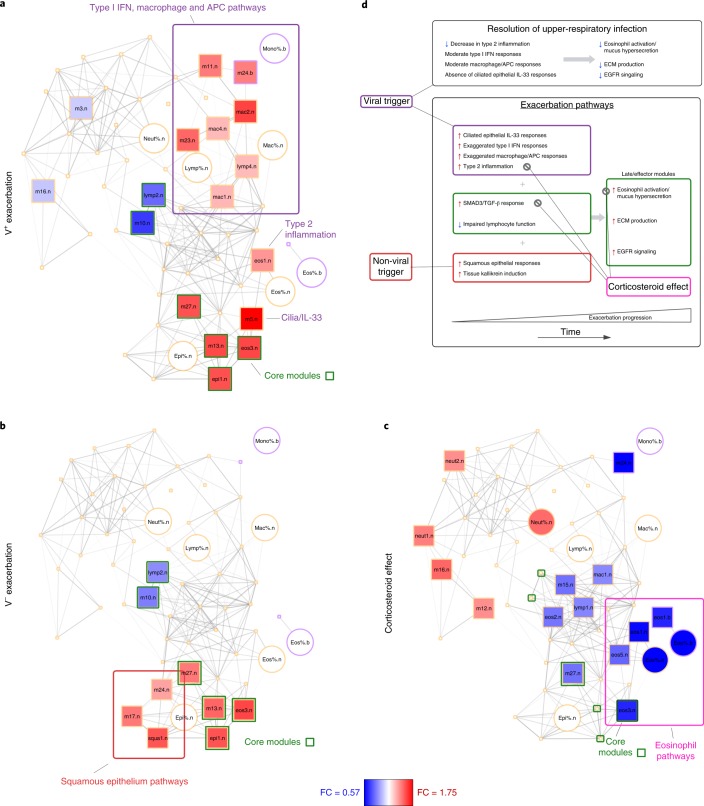
Respiratory infections are common precursors to asthma exacerbations in children, but molecular immune responses that determine whether and how an infection causes an exacerbation are poorly understood. By using systems-scale network analysis, we identify repertoires of cellular transcriptional pathways that lead to and underlie distinct patterns of asthma exacerbation. Specifically, in both virus-associated and nonviral exacerbations, we demonstrate a set of core exacerbation modules, among which epithelial-associated SMAD3 signaling is upregulated and lymphocyte response pathways are downregulated early in exacerbation, followed by later upregulation of effector pathways including epidermal growth factor receptor signaling, extracellular matrix production, mucus hypersecretion, and eosinophil activation. We show an additional set of multiple inflammatory cell pathways involved in virus-associated exacerbations, in contrast to squamous cell pathways associated with nonviral exacerbations. Our work introduces an in vivo molecular platform to investigate, in a clinical setting, both the mechanisms of disease pathogenesis and therapeutic targets to modify exacerbations.
Conflict of interest statement
M.A.G. reports consulting fees from the American Academy of Allergy, Asthma, and Immunology and the American Academy of Pediatrics. A.H.L. reports consulting fees from Merck Sharp & Dohme and reports data-monitoring committee membership for an asthma study conducted by GlaxoSmithKline. R.S.G. reports employment as a special government employee with the Center for Biologics Evaluation and Research and consulting fees from the Consulting Massachusetts Medical Society. G.T.O. reports consulting fees from AstraZeneca and reports a grant from Janssen Pharmaceuticals paid to his employing institution. J.A.P. reports provision of study drugs from GlaxoSmithKline, Teva, Merck, Boehringer-Ingelheim, and Genentech/Novartis for research studies outside of the scope of the submitted work. C.M.K. reports consulting fees from GlaxoSmithKline. E.M.Z. reports consulting fees from Wayne State University. S.J.T. reports consulting fees from Novartis, grants from PCORI, the Fight for Children Foundation, EJF Philanthropies, and NIH/NHLBI, and royalties from Uptodate. M.K. reports consulting fees from Novartis. L.B.B. reports consulting fees from Aerocrine, GlaxoSmithKline, Genentech/Novartis, Merck, Cephalon, DBV Technologies, Teva, Boehringer-Ingelheim, AstraZeneca, WebMD/Medscape, Sanofi, Vectura, and Circassia. J.E.G. reports consulting fees from Janssen, Regeneron, and PReP Biosciences and travel expenses from Boehringer-Ingelheim. W.W.B. reports consulting fees from Boston Scientific, ICON, Novartis, GlaxoSmithKline, Genentech, Roche, Boehringer-Ingelheim, Sanofi Genzyme, AstraZeneca, Teva, 3M, PrEPBiopharm, Circassia, Regeneron, Peptinnovate, and Elsevier. D.J.J. reports consulting fees from Novartis, GlaxoSmithKline, Boehringer-Ingelheim, Pfizer, Commense, and Vectura and a grant from NIH/NHLBI. M.C.A., D.C.B., E.W., B.S., B.J., G.K.K.H., C.C.J., A.B., S.M.S., S.P., P.J.G., L.M.W., and A.T. have nothing to disclose.
Figures
References
Publication types
MeSH terms
Grants and funding
- UL1TR002345 /NH/NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- UL1 TR001105/TR/NCATS NIH HHS/United States
- 1UL1TR001430 /NH/NIH HHS/United States
- UM2 AI117870/AI/NIAID NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- UL1 TR001876 /NH/NIH HHS/United States
- UL1TR001082 /NH/NIH HHS/United States
- UL1 TR001876/TR/NCATS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- UL1TR000451 /NH/NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- UL1 TR000451/TR/NCATS NIH HHS/United States
- UM1 AI114271/AI/NIAID NIH HHS/United States
- 5UM1AI114271 /NH/NIH HHS/United States
- UL1TR001422 /NH/NIH HHS/United States
- 5UL1TR001425 /NH/NIH HHS/United States
- UL1TR000150 /NH/NIH HHS/United States
- UL1 TR001430/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
