

BabyGel pilot: a pilot cluster randomised trial of the provision of alcohol handgel to postpartum mothers to prevent neonatal and young infant infection-related morbidity in the community
- PMID: 30962946
- PMCID: PMC6436217
- DOI: 10.1186/s40814-019-0432-7
BabyGel pilot: a pilot cluster randomised trial of the provision of alcohol handgel to postpartum mothers to prevent neonatal and young infant infection-related morbidity in the community
Abstract
Background: Alcohol-based hand rub (ABHR) is widely used in both health and social facilities to prevent infection, but it is not known whether supplying it for regular perinatal use can prevent newborn sepsis in African rural homes. Our study piloted a cluster randomised trial of providing ABHR to postpartum mothers to prevent neonatal infection-related morbidity in the communities.
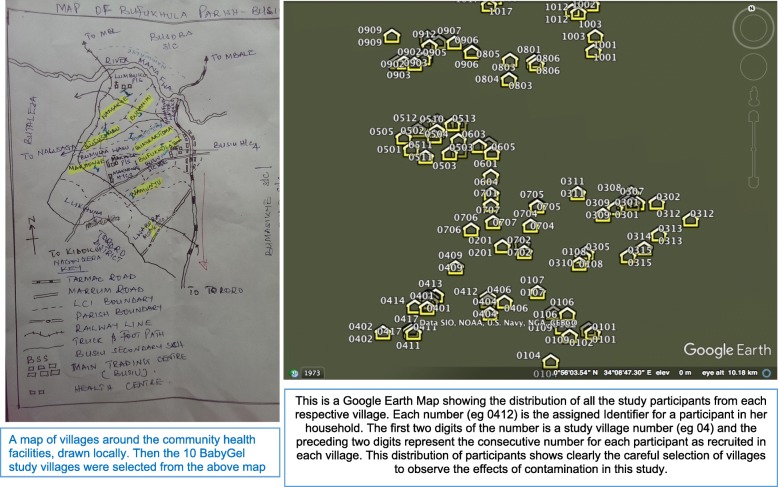
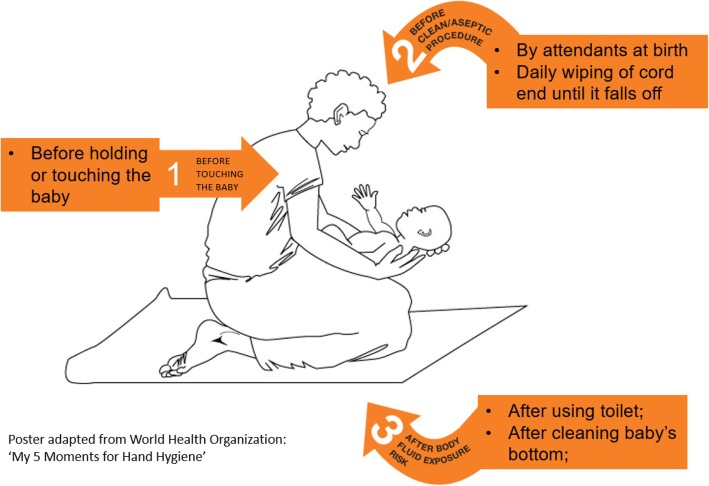
Methods: We conducted a pilot parallel cluster randomised controlled trial across ten villages (clusters) in rural Eastern Uganda. Pregnant women of over 34 weeks' gestation were recruited over a period of 3 months. Both clusters received the standard of care of antenatal health education, Maama Kit, and clinic appointments. In addition, women in the intervention villages received ABHR, instructions on ABHR use, a poster on the 'three moments of hand hygiene', and training. We followed up each mother-baby pair for 3 months after birth and measured rates of consent, recruitment, and follow-up (our target rate was more than 80%). Other measures included ABHR use (the acceptable use was more than four times a day) and its mode of distribution (village health workers (VHWs) or pharmacy), acceptability of study protocol and electronic data capture, and the use of WHO Integrated Management of Childhood Illness (IMCI) tool to screen for newborn infection.
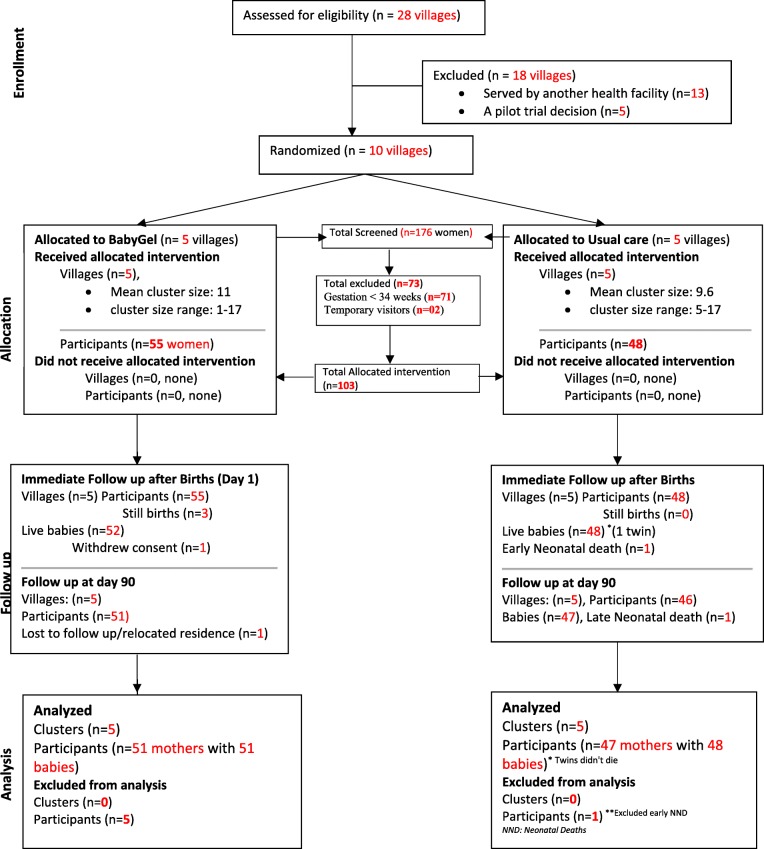
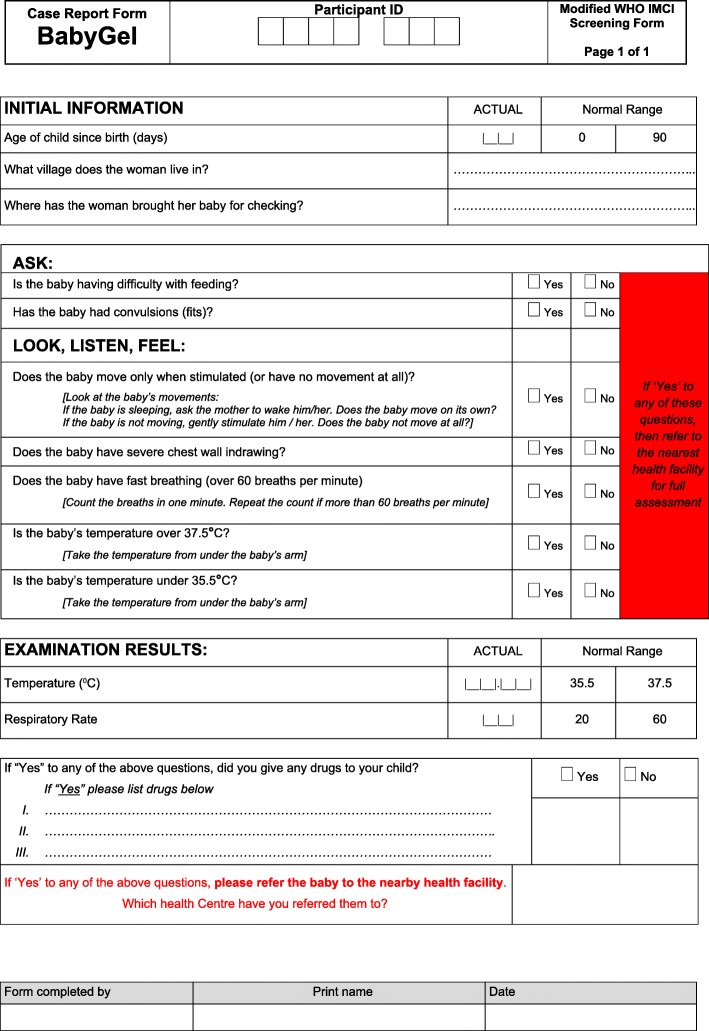
Results: We selected 36% (10/28) of villages for randomisation to either intervention or control. Over 12 weeks, 176 pregnant women were screened and 58.5% (103/176) were eligible. All, 100% (103/103), eligible women gave consent and were enrolled into the trial (55 intervention and 48 control). After birth, 94.5% (52/55) of mothers in the intervention and 100% (48/48) of mothers in the control villages were followed up within 72 h. Most, 90.9% (50/55), of the mothers in the intervention villages (96.2% of live births) and 95.8% (46/48) of mothers in the control villages (95.9% of live births) were followed up at 3 months. In intervention villages, the average hand rub use was 6.6 times per day. VHWs accounted for all ABHR stock, compared to the pharmacy that could not account for 5 l of ABHR. The screening tool was positive for infection among a third of babies, i.e. 29.2% (14/48) in the intervention villages versus 31.4% (16/51) in the control villages.VHWs completed the first four questions of IMCI screening tool with ease and accuracy. There were no adverse reactions with the ABHR.
Conclusion: It is feasible to conduct a cluster-randomised controlled trial (cRCT) of the provision of ABHR to postpartum mothers to prevent neonatal infection-related morbidity in the community in resource-poor settings. Our results indicate that home recruitment promotes excellent follow-up and retention of participants in community trials. The intervention was safe. This pilot study informed the substantial changes necessary in the larger cRCT, including a change in the primary outcome to a composite outcome considering multiple methods of infection detection. A large BabyGel cluster randomised controlled trial is now required.
Trial registration: ISRCTN67852437, registered March 02, 2015.
Trial funding: Medical Research Council/WellcomeTrust/DfID (Global Health Trials Scheme).
Keywords: BabyGel; Hand hygiene; Infant sepsis; Infection; Morbidity alcohol-based hand rub; Mothers; Pilot trial.
Conflict of interest statement
The study was approved by the Mbale Regional Hospital Institutional Review Committee (REIRC IN – COM 011/2015), the University of Liverpool Research and Ethics Committee (RETH000808), and the Uganda National Council for Science and Technology (HS1768). Informed consent for participation in the pilot trial was obtained from all participants before recruitment. The study was registered with the ISRCTN registry (ISRCTN 67852437).Not ApplicableThe authors declare that they have no competing interests (financial or non-financial). Saraya Uganda Ltd. provided the ABHR free of charge but had no input into the study design, conduct, analysis, or interpretation.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- You D, et al. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet. 2015;386(10010):2275–2286. doi: 10.1016/S0140-6736(15)00120-8. - DOI - PubMed
-
- WHO/UNICEF . Ending preventable child deaths from pneumonia and diarrhoea by 2025. New York: The integrated global action plan for pneumonia and diarrhoea (GAPPD); 2013. - PubMed
-
- UNICEF. One is too many: ending child deaths from pneumonia and diarrhoea. New York: United Nations Children’s Fund (UNICEF); 2016.
Grants and funding
LinkOut - more resources
Full Text Sources
