

A comparison of peri-operative outcomes between elective and non-elective total hip arthroplasties
- PMID: 30963073
- PMCID: PMC6409228
- DOI: 10.21037/atm.2019.01.64
A comparison of peri-operative outcomes between elective and non-elective total hip arthroplasties
Abstract
Background: Elective total hip arthroplasties (THAs) entail a more extensive pre-operative planning process compared to non-elective THAs and this may contribute to a disparity in outcomes. However, the differences in peri- and post-operative outcomes between elective and non-elective THAs remain unclear. Therefore, the purpose of this study was to: (I) determine nationwide trends in operative times and (II) evaluate the association between surgery type, elective or non-elective with respect to (I) operative times; (II) hospital lengths-of-stay (LOS); (III) discharge disposition; (IV) 30-day post-operative complications; (V) reoperations; and (VI) readmissions.
Methods: The NSQIP database was queried for all primary THAs (CPT code 27130) performed between 2011 and 2016. This yielded 130,261 cases, which were then stratified into elective (n=125,293) and non-elective (n=4,968) cases. One-way analysis of variance (ANOVA) were used to evaluate the associations between operative times and surgery year. Univariate analyses of surgery type with the following outcomes of interest were also performed: operative times, LOS, and discharge disposition as well as 30-day complication, reoperation, and readmission rates. A multiple linear regression model was used to evaluate the relationships of operative times and LOS with surgery types after adjusting for surgery year and patient factors [age, sex, body mass index (BMI), and American Society of Anesthesiologists (ASA) score]. A log-transformed dependent variable was used to calculate the percentage difference in mean operative times and LOS. Multivariate logistic regression models adjusted for patient factors and year of surgery were used to evaluate associations of surgery type with complication, reoperation, and readmission rates.
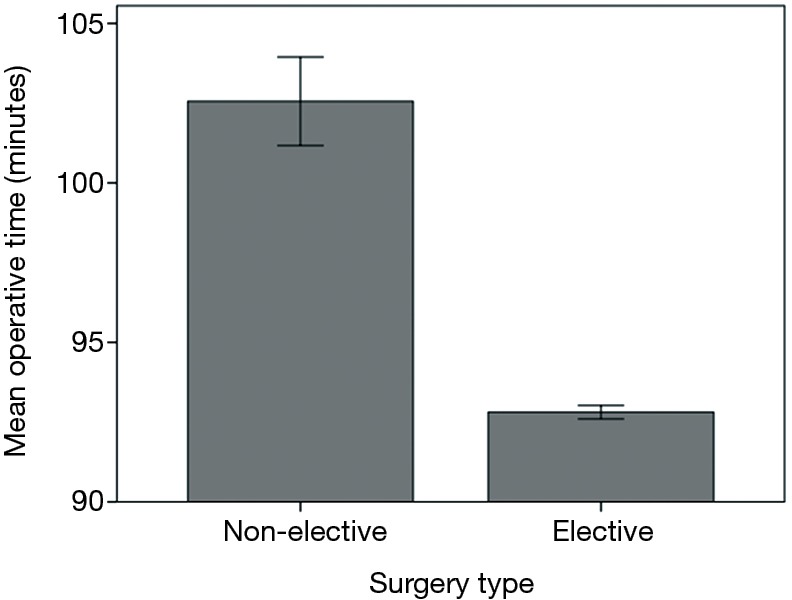
Results: Over the 6-year period, mean operative times (93 vs. 103 minutes, P<0.001) and LOS (3 vs. 6 days, P<0.001) were significantly shorter in elective cases compared to non-elective cases. The relationships between operative times or LOS and surgery type remained significant even after adjusting for age, sex, BMI, ASA, and year of surgery (P<0.001). Compared to the non-elective cohort, patients in the elective cohort were more likely to be discharged home (74% vs. 69%, P<0.001). Elective patients had lower rates of several 30-day complications including deep SSI (P<0.001), transfusions (P<0.001), sepsis (P<0.001), and readmission (P<0.005) compared to non-elective patients. These associations remained significant after accounting for potential confounders with multivariate logistic regression.
Conclusions: Findings from this study showed that elective THAs, in which there is more potential for pre-operative planning, were associated with shorter operative times and LOS, as well as fewer complication and readmission rates. These results likely reflect the development of more efficient surgical techniques and improved pre- and intra-operative planning guides.
Keywords: Elective cases; non-elective cases; outcomes; pre-operative planning; total hip arthroplasty (THA).
Conflict of interest statement
Conflicts of Interest: MA Mont: AAOS, Cymedica, DJ Orthopaedics, Johnson & Johnson, Journal of Arthroplasty, Journal of Knee Surgery, Microport, National Institutes of Health (NIAMS & NICHD), Ongoing Care Solutions, Orthopedics, Orthosensor, Pacira, Peerwell, Performance Dynamics Inc, Sage, Stryker: IP royalties, Surgical Technologies International, Kolon TissueGene. The other authors have no conflicts of interest to declare.
Figures

References
-
- Padegimas EM, Verma K, Zmistowski B, et al. Medicare Reimbursement for Total Joint Arthroplasty: The Driving Forces. J Bone Joint Surg Am 2006;98:1007-13. - PubMed
-
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007;89:780-5. - PubMed
LinkOut - more resources
Full Text Sources