

The role of the opioid system in decision making and cognitive control: A review
- PMID: 30963411
- PMCID: PMC6599188
- DOI: 10.3758/s13415-019-00710-6
The role of the opioid system in decision making and cognitive control: A review
Abstract
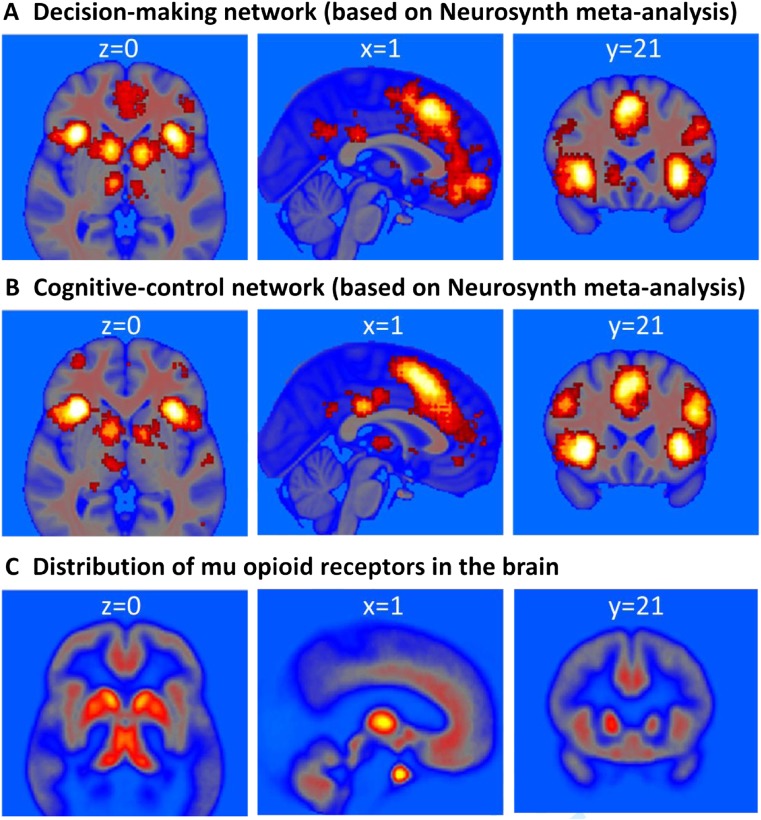
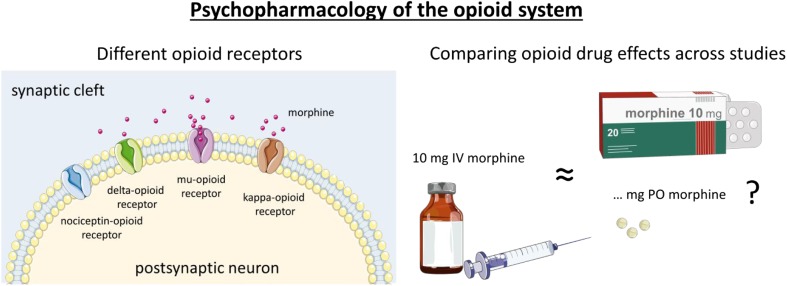
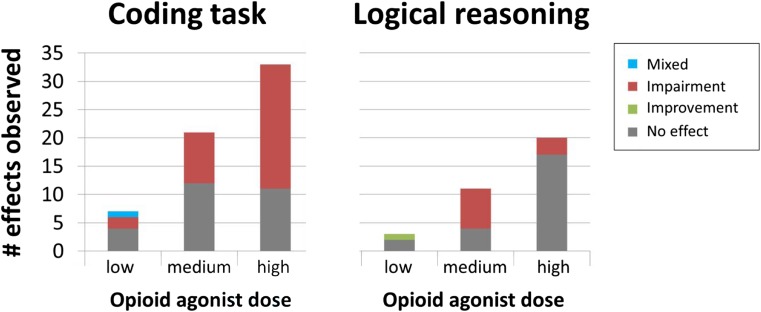
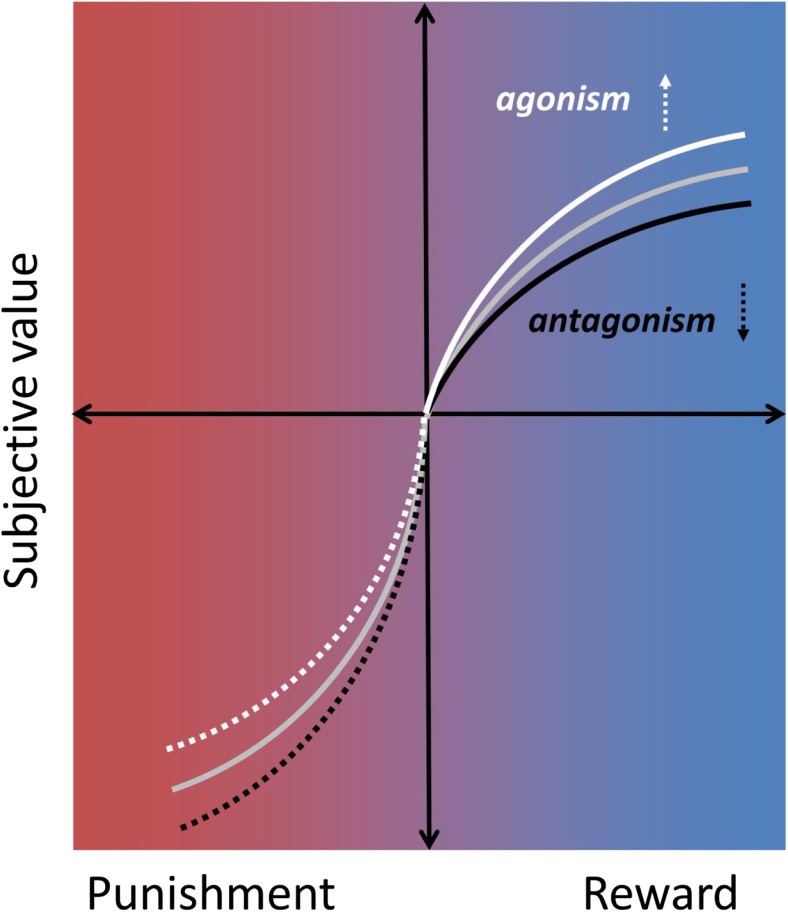
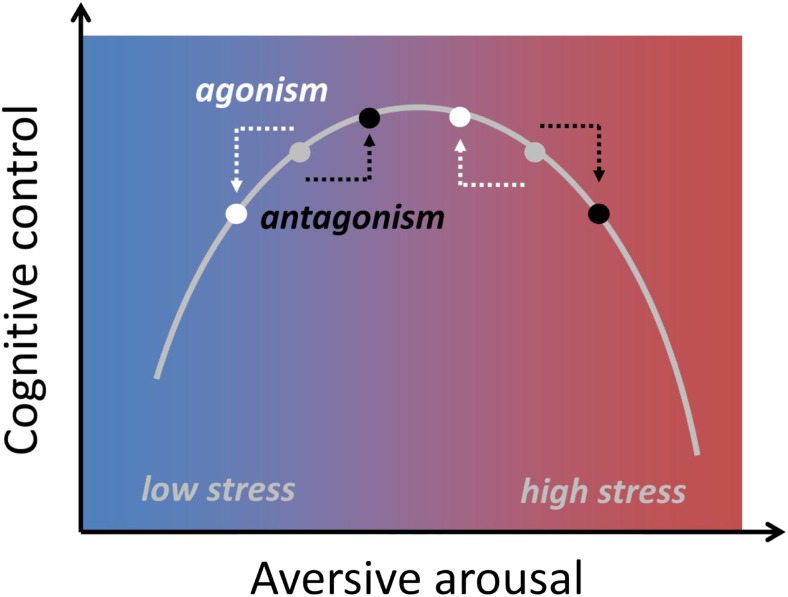
The opioid system regulates affective processing, including pain, pleasure, and reward. Restricting the role of this system to hedonic modulation may be an underestimation, however. Opioid receptors are distributed widely in the human brain, including the more "cognitive" regions in the frontal and parietal lobes. Nonhuman animal research points to opioid modulation of cognitive and decision-making processes. We review emerging evidence on whether acute opioid drug modulation in healthy humans can influence cognitive function, such as how we choose between actions of different values and how we control our behavior in the face of distracting information. Specifically, we review studies employing opioid agonists or antagonists together with experimental paradigms of reward-based decision making, impulsivity, executive functioning, attention, inhibition, and effort. Although this field is still in its infancy, the emerging picture suggests that the mu-opioid system can influence higher-level cognitive function via modulation of valuation, motivation, and control circuits dense in mu-opioid receptors, including orbitofrontal cortex, basal ganglia, amygdalae, anterior cingulate cortex, and prefrontal cortex. The framework that we put forward proposes that opioids influence decision making and cognitive control by increasing the subjective value of reward and reducing aversive arousal. We highlight potential mechanisms that might underlie the effects of mu-opioid signaling on decision making and cognitive control and provide directions for future research.
Keywords: Affect; Cognitive control; Decision making; Drugs; Executive function; Hedonic states; Mood; Morphine; Mu-opioid receptors; Opioid system; Reward; Value-based choice.
Figures
References
-
- Allen ME, Coen D. Naloxone blooking of running-induced mood changes. Annals of Sports Medicine. 1987;3:190–195.
-
- Anderson WS, Sheth RN, Bencherif B, Frost JJ, Campbell JN. Naloxone increases pain induced by topical capsaicin in healthy human volunteers. Pain. 2002;99:207–216. - PubMed
-
- Arnsten AFT, Segal DS, Loughlin SE, Roberts DCS, Jolla L, Diego S. Evidence for an interaction of opioid and noradrenergic locus coeruleus systems in the regulation of environmental stimulus-directed behavior. Brain Research. 1981;222:351–363. - PubMed
-
- Arnsten AFT, Segal DS, Neville HJ, Hillyard SA, Janowsky DS, Judd LL, Bloom FE. Naloxone augments electrophysiological signs of selective attention in man. Nature. 1983;304:725–727. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
