

Knowledge-based planning for intensity-modulated radiation therapy: A review of data-driven approaches
- PMID: 30963580
- PMCID: PMC6561807
- DOI: 10.1002/mp.13526
Knowledge-based planning for intensity-modulated radiation therapy: A review of data-driven approaches
Abstract
Purpose: Intensity-Modulated Radiation Therapy (IMRT), including its variations (including IMRT, Volumetric Arc Therapy (VMAT), and Tomotherapy), is a widely used and critically important technology for cancer treatment. It is a knowledge-intensive technology due not only to its own technical complexity, but also to the inherently conflicting nature of maximizing tumor control while minimizing normal organ damage. As IMRT experience and especially the carefully designed clinical plan data are accumulated during the past two decades, a new set of methods commonly termed knowledge-based planning (KBP) have been developed that aim to improve the quality and efficiency of IMRT planning by learning from the database of past clinical plans. Some of this development has led to commercial products recently that allowed the investigation of KBP in numerous clinical applications. In this literature review, we will attempt to present a summary of published methods of knowledge-based approaches in IMRT and recent clinical validation results.
Methods: In March 2018, a literature search was conducted in the NIH Medline database using the PubMed interface to identify publications that describe methods and validations related to KBP in IMRT including variations such as VMAT and Tomotherapy. The search criteria were designed to have a broad scope to capture relevant results with high sensitivity. The authors filtered down the search results according to a predefined selection criteria by reviewing the titles and abstracts first and then by reviewing the full text. A few papers were added to the list based on the references of the reviewed papers. The final set of papers was reviewed and summarized here.
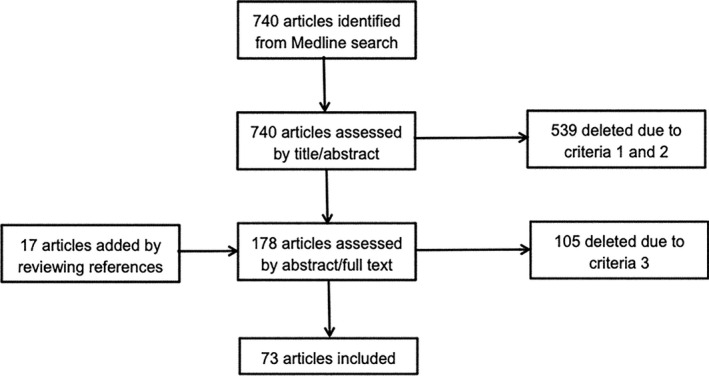
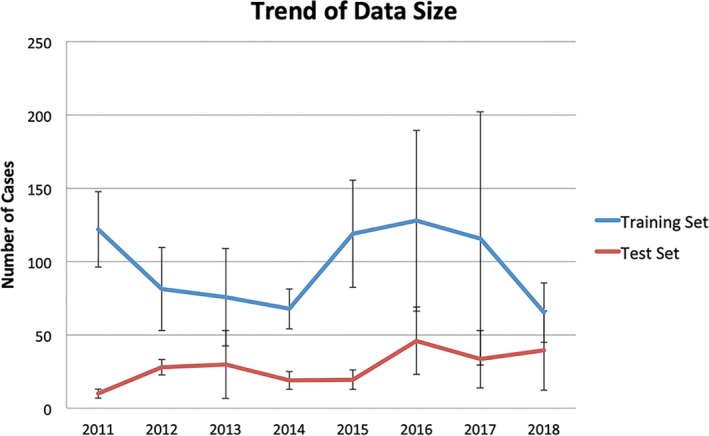
Results: The initial search yielded a total of 740 articles. A careful review of the titles, abstracts, and eventually the full text and then adding relevant articles from reviewing the references resulted in a final list of 73 articles published between 2011 and early 2018. These articles described methods for developing knowledge models for predicting such parameters as dosimetric and dose-volume points, voxel-level doses, and objective function weights that improve or automate IMRT planning for various cancer sites, addressing different clinical and quality assurance needs, and using a variety of machine learning approaches. A number of articles reported carefully designed clinical studies that assessed the performance of KBP models in realistic clinical applications. Overwhelming majority of the studies demonstrated the benefits of KBP in achieving comparable and often improved quality of IMRT planning while reducing planning time and plan quality variation.
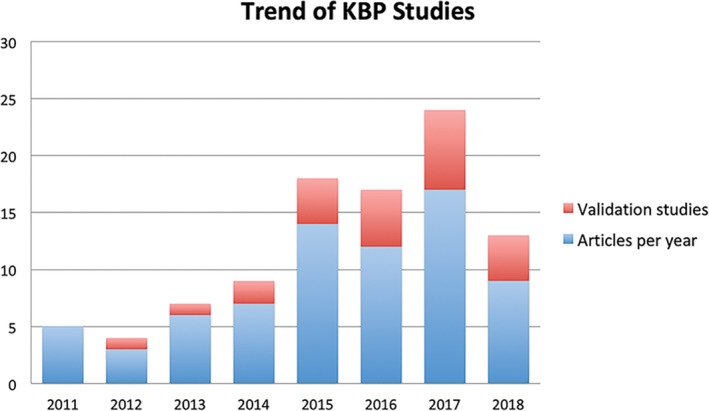
Conclusions: The number of KBP-related studies has been steadily increasing since 2011 indicating a growing interest in applying this approach to clinical applications. Validation studies have generally shown KBP to produce plans with quality comparable to expert planners while reducing the time and efforts to generate plans. However, current studies are mostly retrospective and leverage relatively small datasets. Larger datasets collected through multi-institutional collaboration will enable the development of more advanced models to further improve the performance of KBP in complex clinical cases. Prospective studies will be an important next step toward widespread adoption of this exciting technology.
Keywords: IMRT; KBP; VMAT; IMRT planning; intensity-modulated radiation therapy; knowledge modeling; knowledge-based planning; machine learning; tomotherapy.
© 2019 The Authors. Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors do not have relevant conflicts of interest to disclose.
Figures
References
-
- Kalet IJ, Paluszynski W. Knowledge‐based computer systems for radiotherapy planning. Am J Clin Oncol. 1990;13:344–351. - PubMed
-
- Shwe MA, Tu SW, Fagan LM. Validating the knowledge base of a therapy planning system. Methods Inf Med. 1989;28:36–50. - PubMed
-
- Zhang X, Li X, Quan EM, Pan X, Li Y. A methodology for automatic intensity‐modulated radiation treatment planning for lung cancer. Phys Med Biol, 2011;56:3873. - PubMed
-
- Voet PW, Dirkx ML, Breedveld S, Fransen D, Levendag PC, Heijmen BJ. Toward fully automated multicriterial plan generation: a prospective clinical study. Int J Radiat Oncol Biol Phys. 2013;85:866–872. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
