

Bone Marrow Mesenchymal Stromal Cell Treatment in Patients with Osteoarthritis Results in Overall Improvement in Pain and Symptoms and Reduces Synovial Inflammation
- PMID: 30964245
- PMCID: PMC6646697
- DOI: 10.1002/sctm.18-0183
Bone Marrow Mesenchymal Stromal Cell Treatment in Patients with Osteoarthritis Results in Overall Improvement in Pain and Symptoms and Reduces Synovial Inflammation
Abstract
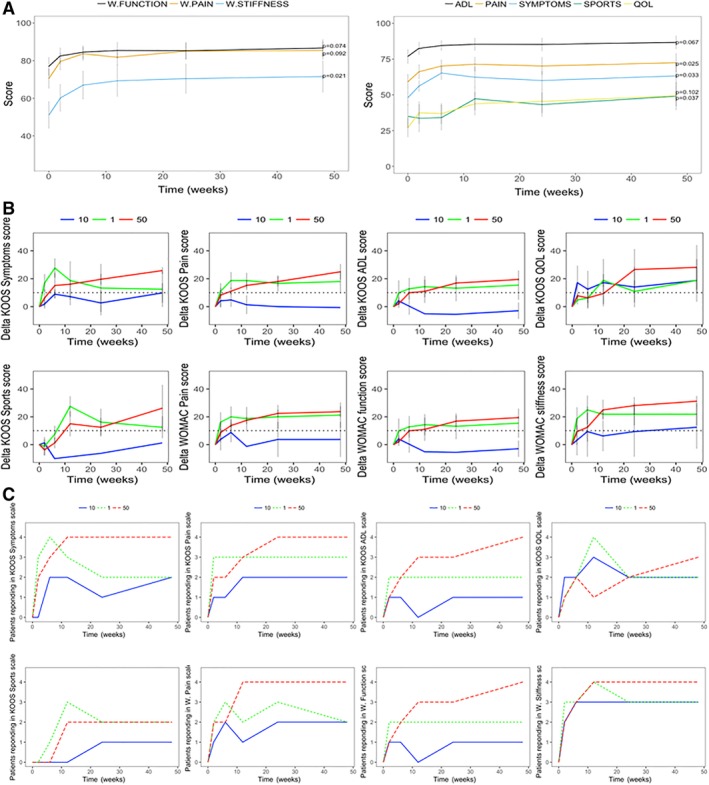
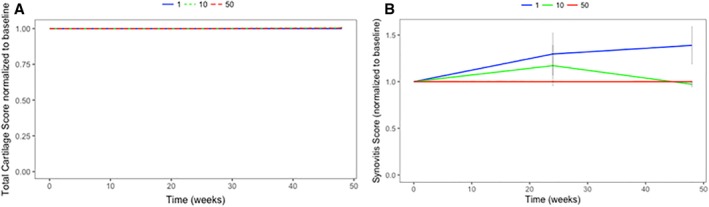
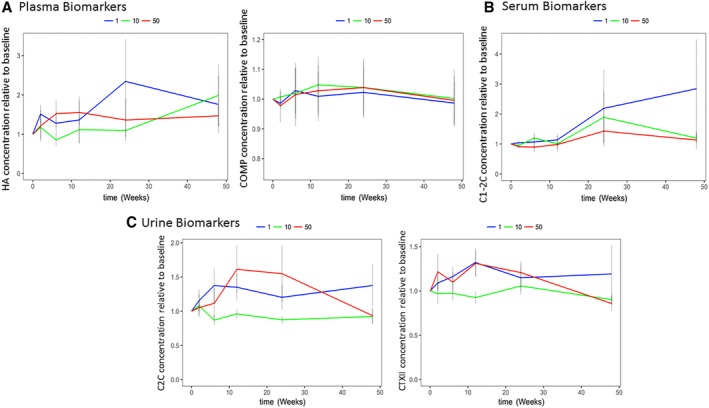
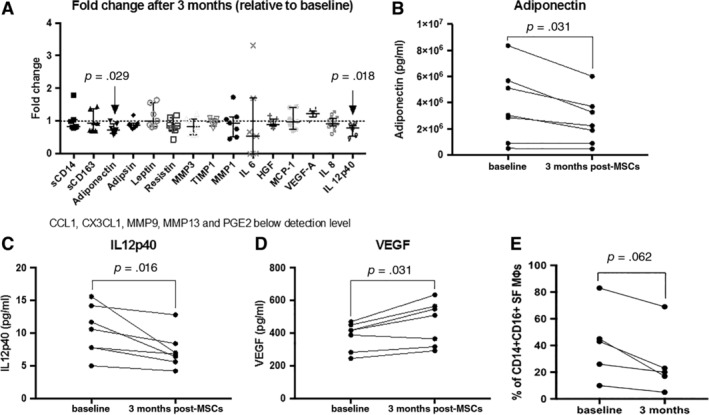
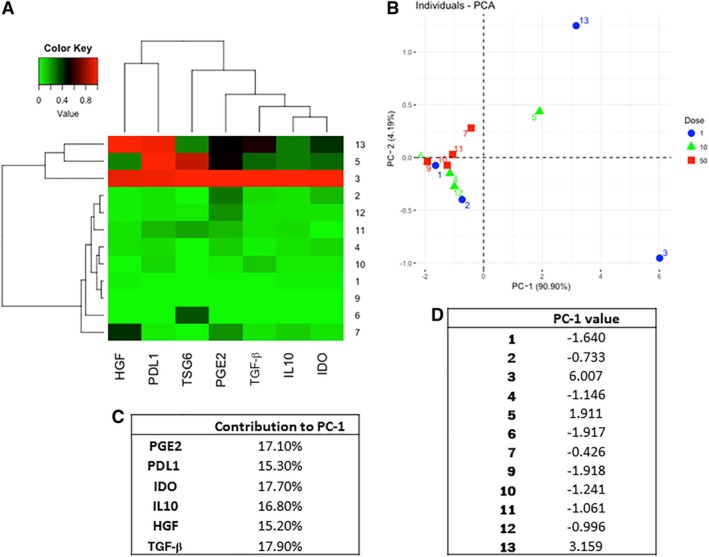
Patients with late-stage Kellgren-Lawrence knee osteoarthritis received a single intra-articular injection of 1, 10, or 50 million bone marrow mesenchymal stromal cells (BM-MSCs) in a phase I/IIa trial to assess safety and efficacy using a broad toolset of analytical methods. Besides safety, outcomes included patient-reported outcome measures (PROMs): Knee Injury and Osteoarthritis Outcome Score (KOOS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC); contrast-enhanced magnetic resonance imaging (MRI) for cartilage morphology (Whole Organ MRI Scores [WORMS]), collagen content (T2 scores), and synovitis; and inflammation and cartilage turnover biomarkers, all over 12 months. BM-MSCs were characterized by a panel of anti-inflammatory markers to predict clinical efficacy. There were no serious adverse events, although four patients had minor, transient adverse events. There were significant overall improvements in KOOS pain, symptoms, quality of life, and WOMAC stiffness relative to baseline; the 50 million dose achieved clinically relevant improvements across most PROMs. WORMS and T2 scores did not change relative to baseline. However, cartilage catabolic biomarkers and MRI synovitis were significantly lower at higher doses. Pro-inflammatory monocytes/macrophages and interleukin 12 levels decreased in the synovial fluid after MSC injection. The panel of BM-MSC anti-inflammatory markers was strongly predictive of PROMs over 12 months. Autologous BM-MSCs are safe and result in significant improvements in PROMs at 12 months. Our analytical tools provide important insights into BM-MSC dosing and BM-MSC reduction of synovial inflammation and cartilage degradation and provide a highly predictive donor selection criterion that will be critical in translating MSC therapy for osteoarthritis. Stem Cells Translational Medicine 2019;8:746&757.
Keywords: Arthritis; Cellular therapy; Clinical trials; Mesenchymal stem cells; Monocyte; Selectable marker.
© 2019 The Authors. Stem Cells Translational Medicine published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Conflict of interest statement
A.G.‐A. declared employment and stock ownership interest with Bluerock Therapeutics. K.A.S. declared advisory role for Sanofi Canada and honoraria from Sanofi Canada. S.V. declared consulting and advising for Stem Cell Network, CellCAN, and OIRM and research funding from NSERC and OIRM (not to support this study). The other authors indicated no potential conflicts of interest.
Figures
References
-
- Bombardier C, Hawker G, Mosher D. The Impact of Arthritis in Canada, Arthritis Alliance of Canada, Toronto, Ontario, Canada: Today and Over 30 Years, 2011.
-
- Vega A, Martin‐Ferrero MA, Del Canto F et al. Treatment of knee osteoarthritis with allogeneic bone marrow mesenchymal stem cells: A randomized controlled trial. Transplantation 2015;99:1681–1690. - PubMed
-
- Orozco L, Munar A, Soler R et al. Treatment of knee osteoarthritis with autologous mesenchymal stem cells: A pilot study. Transplantation 2013;95:1535–1541. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
