

Immunologic Consequences of Sequencing Cancer Radiotherapy and Surgery
- PMID: 30964698
- PMCID: PMC6661069
- DOI: 10.1200/CCI.18.00075
Immunologic Consequences of Sequencing Cancer Radiotherapy and Surgery
Abstract
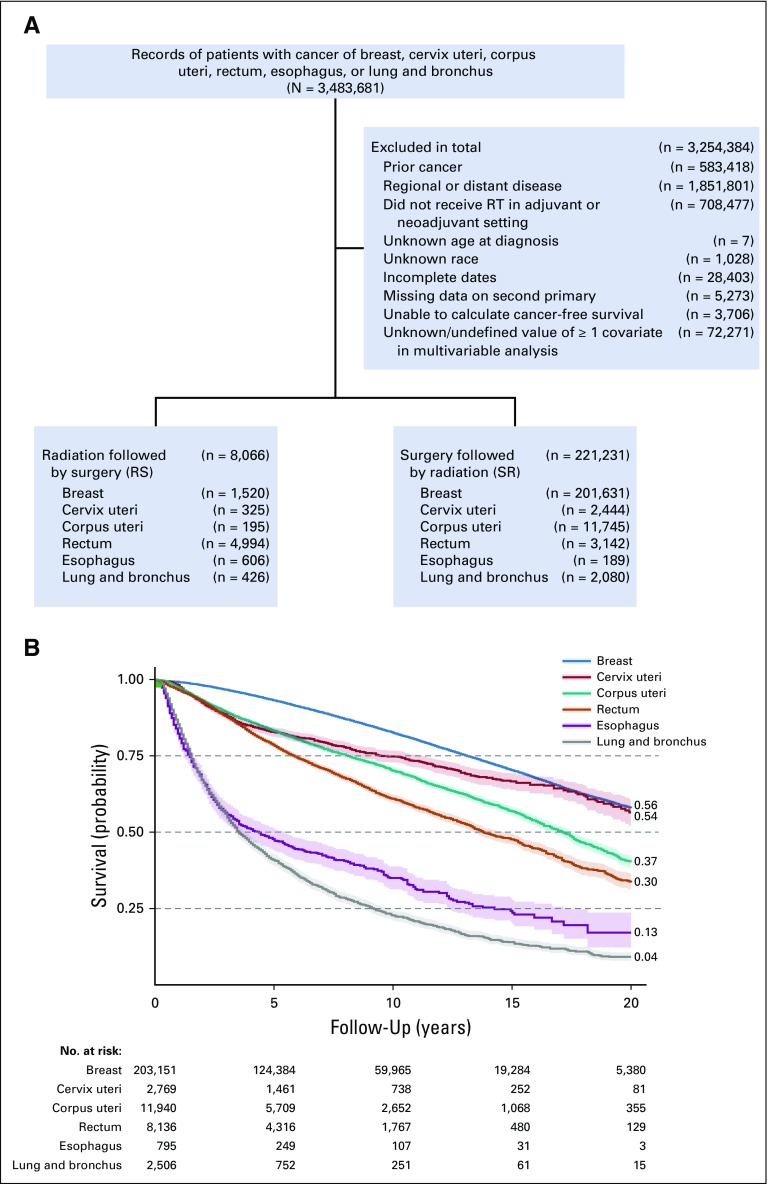
Purpose: Early-stage cancers are routinely treated with surgery followed by radiotherapy (SR). Radiotherapy before surgery (RS) has been widely ignored for some cancers. We evaluate overall survival (OS) and disease-free survival (DFS) with SR and RS for different cancer types and simulate the plausibility of RS- and SR-induced antitumor immunity contributing to outcomes.
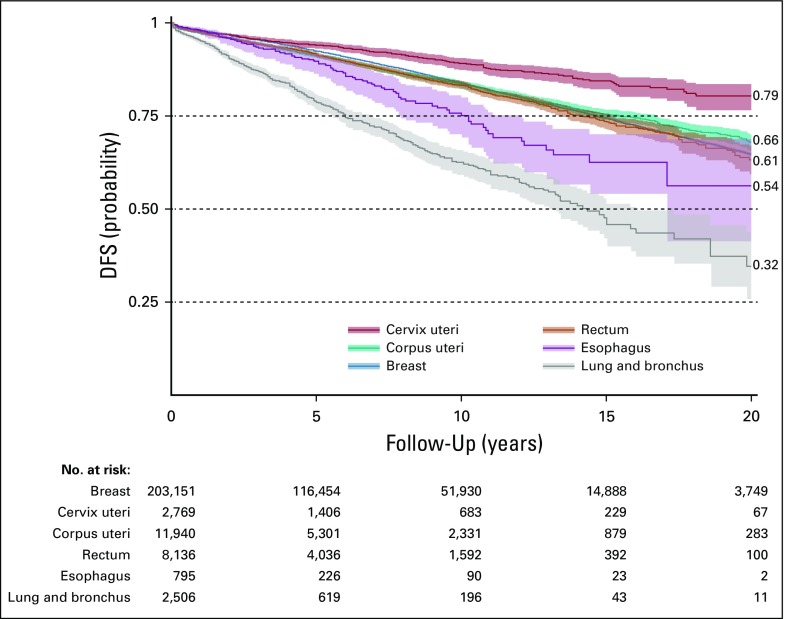
Materials and methods: We analyzed a SEER data set of early-stage cancers treated with SR or RS. OS and DFS were calculated for cancers with sufficient numbers for statistical power (cancers of lung and bronchus, esophagus, rectum, cervix uteri, corpus uteri, and breast). We simulated the immunologic consequences of SR, RS, and radiotherapy alone in a mathematical model of tumor-immune interactions.
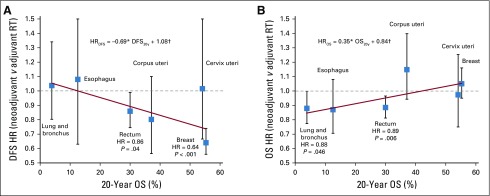
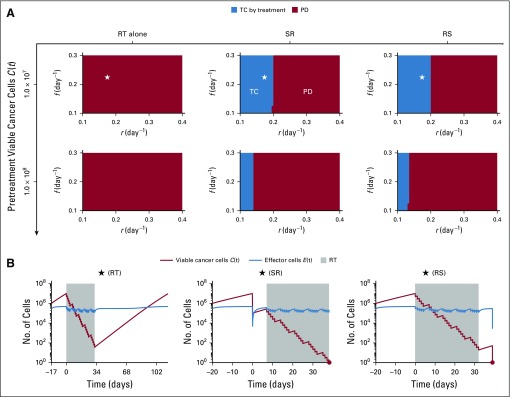
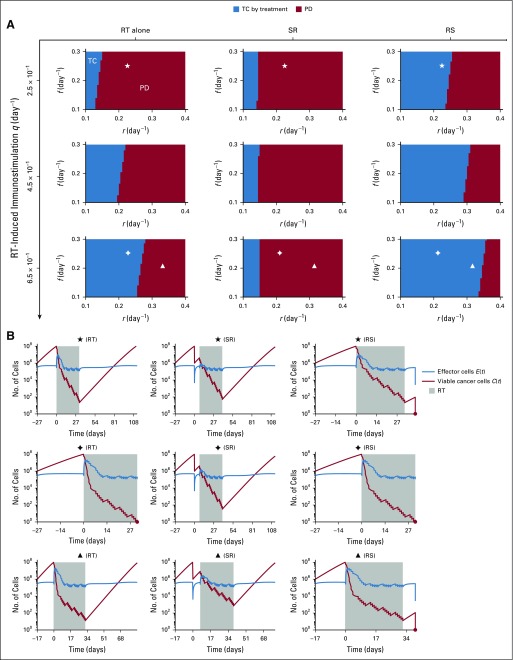
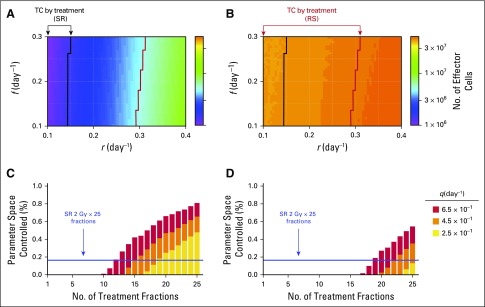
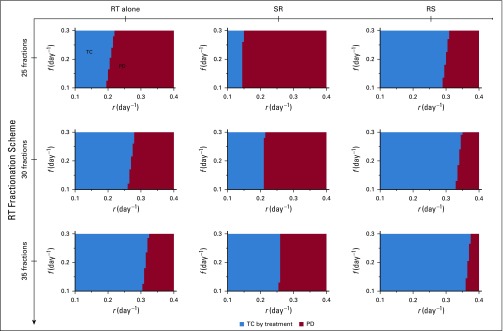
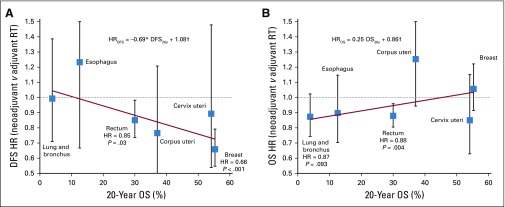
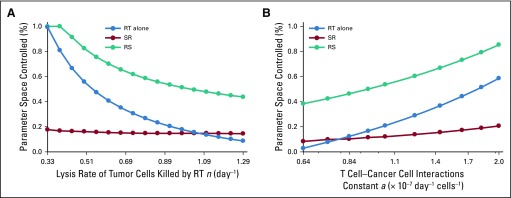
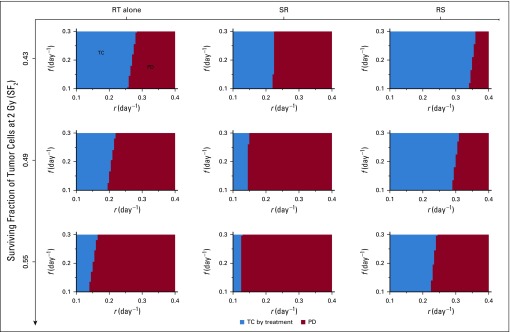
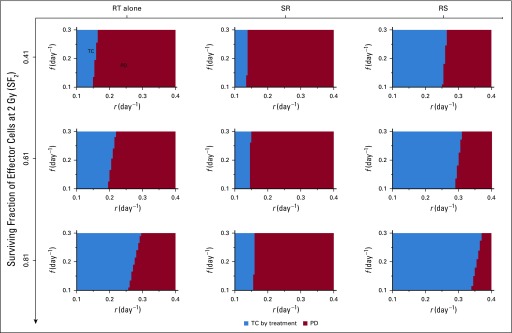
Results: RS improved OS for cancers with low 20-year survival rates (lung: hazard ratio [HR], 0.88; P = .046) and improved DFS for cancers with higher survival (breast: HR = 0.64; P < .001). For rectal cancer, with intermediate 20-year survival, RS improved both OS (HR = 0.89; P = .006) and DFS (HR = 0.86; P = .04). Model simulations suggested that RS could increase OS by eliminating cancer for a broader range of model parameters and radiotherapy-induced antitumor immunity compared with SR for selected parameter combinations. This could create an immune memory that may explain increased DFS after RS for certain cancers.
Conclusion: Study results suggest plausibility that radiation to the bulk of the tumor could induce a more robust immune response and better harness the synergy of radiotherapy and antitumor immunity than postsurgical radiation to the tumor bed. This exploratory study provides motivation for prospective evaluation of immune activation of RS versus SR in controlled clinical studies.
Conflict of interest statement
Jan Poleszczuk
Sungjune Kim
Shari Pilon-Thomas
Jose J. Conejo-Garcia
Hatem Soliman
Brian Czerniecki
Heiko Enderling
No other potential conflicts of interest were reported.
Figures
References
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–1241. - PubMed
-
- Kao J, Lavaf A, Teng MS, et al. Adjuvant radiotherapy and survival for patients with node-positive head and neck cancer: An analysis by primary site and nodal stage. Int J Radiat Oncol Biol Phys. 2008;71:362–370. - PubMed
-
- Creutzberg CL, van Putten WLJ, Wárlám-Rodenhuis CC, et al. Outcome of high-risk stage IC, grade 3, compared with stage I endometrial carcinoma patients: The Postoperative Radiation Therapy in Endometrial Carcinoma trial. J Clin Oncol. 2004;22:1234–1241. - PubMed
-
- Bui DL, Yu JB. Trends in adjuvant and neoadjuvant radiotherapy for cancer treatment from 1973 to 2011. Cancer J. 2015;21:147–149. - PubMed
-
- Frykholm GJ, Glimelius B, Påhlman L. Preoperative or postoperative irradiation in adenocarcinoma of the rectum: Final treatment results of a randomized trial and an evaluation of late secondary effects. Dis Colon Rectum. 1993;36:564–572. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
