

Intratumor heterogeneity of PD-L1 expression in head and neck squamous cell carcinoma
- PMID: 30967647
- PMCID: PMC6734649
- DOI: 10.1038/s41416-019-0449-y
Intratumor heterogeneity of PD-L1 expression in head and neck squamous cell carcinoma
Abstract
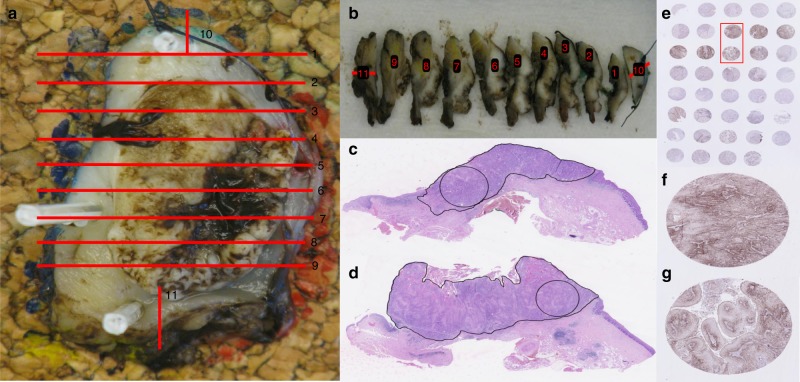
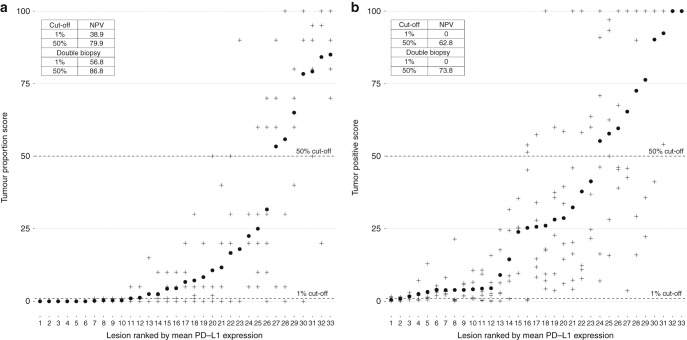
Intratumor heterogeneity may contribute to the ambiguous clinical results on PD-L1 status as a predictor for immunotherapy response in patients with HNSCC. This decreases the utility of PD-L1 expression from single tumour biopsies as a predictive biomarker. In this prospective study, intratumor heterogeneity of PD-L1 expression in HNSCC was investigated with both Tumour Proportion Score (TPS) and Combined Positive Score (CPS). Thirty-three whole surgical specimens from 28 patients with HNSCC were included. PD-L1 expression in six random core biopsies from each surgical specimen was used to assess the concordance between multiple biopsies and the negative predictive value of a single negative core biopsy. With 1% cut off, 36% of the specimens were concordant with TPS and 52% with CPS. With a 50% cut-off value the concordance was 70% with TPS and 55% with CPS. Defining a tumour as positive if just a single-one of the biopsies was positive, the negative predictive value (NPV) of a single negative core biopsy was 38.9 and 0% (1% cut off), and 79.9% and 62.8% (50% cut off) for TPS and CPS, respectively. In conclusion, PD-L1 positivity varies markedly within the tumour, both with TPS and CPS, challenging the utility of this biomarker.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018;81:45–51. doi: 10.1016/j.oraloncology.2018.04.008. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
