

Progression characteristics of ellipsoid zone loss in macular telangiectasia type 2
- PMID: 30968592
- PMCID: PMC6785352
- DOI: 10.1111/aos.14110
Progression characteristics of ellipsoid zone loss in macular telangiectasia type 2
Abstract
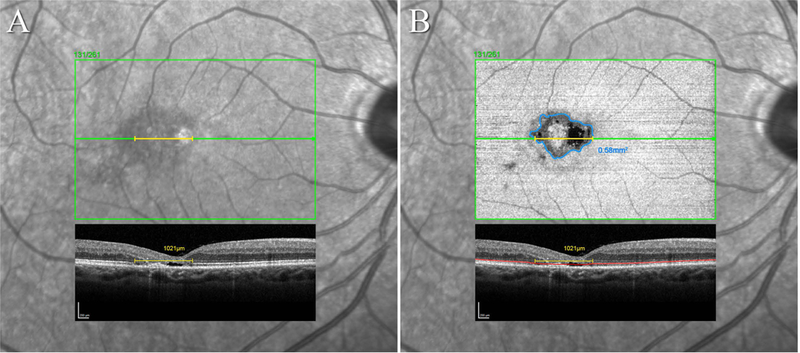
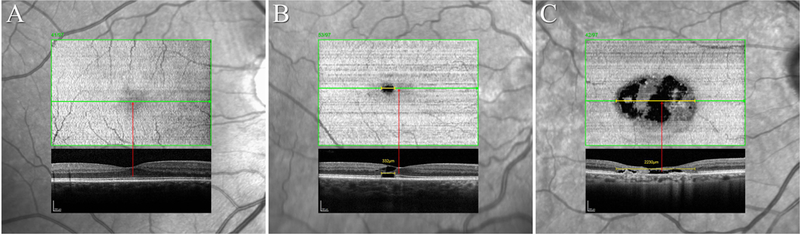
Purpose: To investigate the progression characteristics of ellipsoid zone (EZ) loss in eyes with macular telangiectasia type 2 (MacTel) as reflected by area and linear measurements, and their relevance for visual acuity.
Methods: Participants were selected from the MacTel Study cohort. Linear and area measurements of EZ loss were performed in Spectral-Domain Optical Coherence Tomograph (SD-OCT) volume scans. Progression characteristics and correlations between linear and area measurements were analysed using linear mixed effects models.
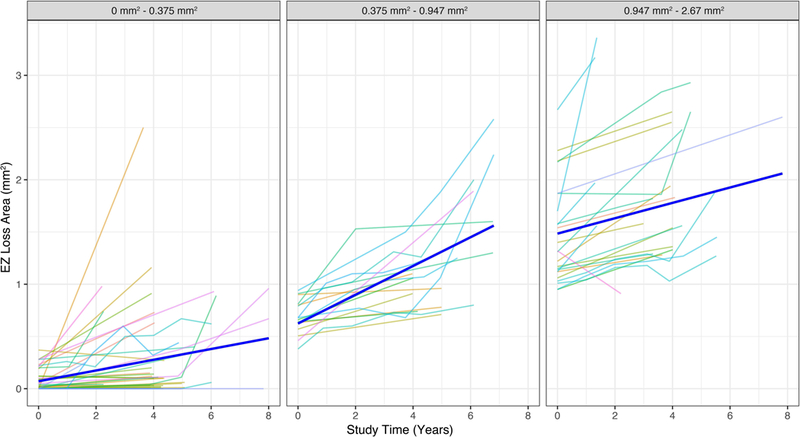
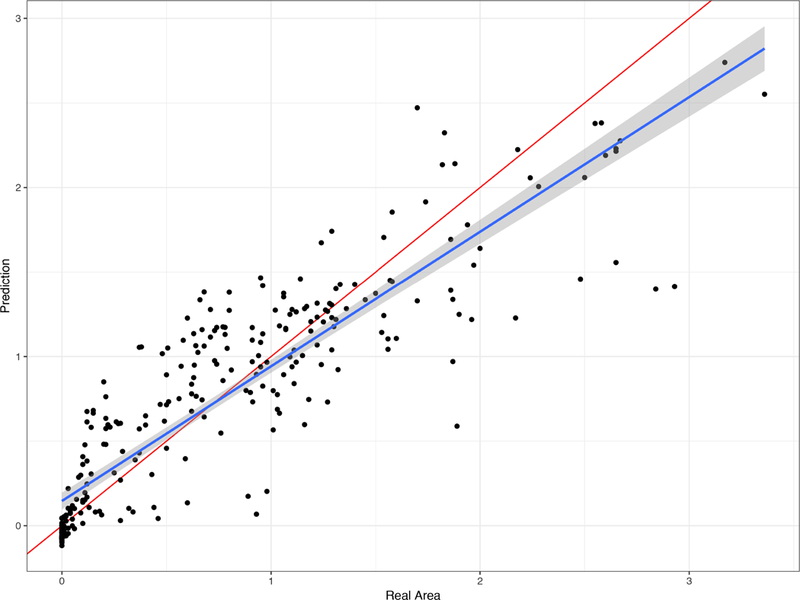
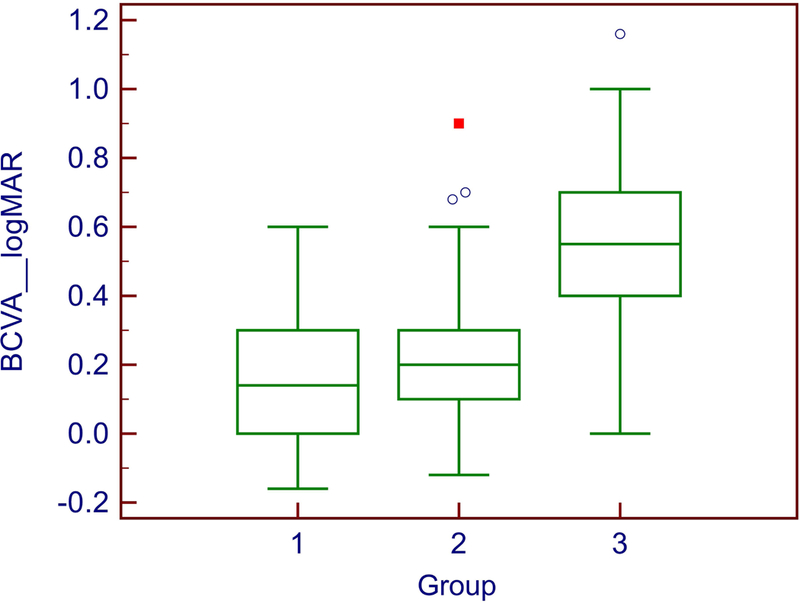
Results: A total of 134 eyes of 70 patients were included (85 eyes with follow-up, mean 4.7 years, range: 1.4-8 years). Ellipsoid zone (EZ) loss significantly progressed at a mean annual increment of 0.057 mm2 (p = 0.005). The progression rate was non-linear and interacted significantly with initial EZ lesion size indicating an exponential growth before reaching a plateau. There was a strong heterogeneity in area sizes between fellow eyes. EZ break length had a significant linear effect on EZ break area (b = 1.06, p < 0.001) and could predict it. The location of the EZ break had a significant impact on visual acuity.
Conclusion: Ellipsoid zone (EZ) loss in MacTel has a non-linear progression characteristic, and its rate depends on area size at baseline, which must be taken into account at sample selection in clinical trials. Our results show a good correlation of linear and area measures of EZ loss and a segregation of best-corrected visual acuity by EZ location, which may help routine clinical practice.
Keywords: OCT; MacTel; ellipsoid zone; en face image; macular telangiectasia type 2.
© 2019 Acta Ophthalmologica Scandinavica Foundation. Published by John Wiley & Sons Ltd.
Figures
References
-
- Charbel Issa P, Berendschot TT, Staurenghi G, Holz FG & Scholl HP(2008): Confocal blue reflectance imaging in type 2 idiopathic macular telangiectasia. Invest Ophthalmol Vis Sci 49: 1172–1177. - PubMed
-
- Clemons TE, Gillies MC, Chew EY, Bird AC, Peto T, Wang JJ, Mitchell P, Ramdas WD& Vingerling JR(2013): Medical characteristics of patients with macular telangiectasia type 2 (MacTel Type 2) MacTel project report no. 3. Ophthalmic Epidemiol 20: 109–113. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
