

Review
doi: 10.1152/physiol.00054.2018.
A Critical Evaluation of Current Concepts in Cerebral Palsy
Affiliations
- PMID: 30968751
- PMCID: PMC7938766
- DOI: 10.1152/physiol.00054.2018
Item in Clipboard
Review
A Critical Evaluation of Current Concepts in Cerebral Palsy
Physiology (Bethesda).
.
Abstract
Spastic cerebral palsy (CP), despite the name, is not consistently identifiable by specific brain lesions. CP animal models focus on risk factors for development of CP, yet few reproduce the diagnostic symptoms. Animal models of CP must advance beyond risk factors to etiologies, including both the brain and spinal cord.
Figures
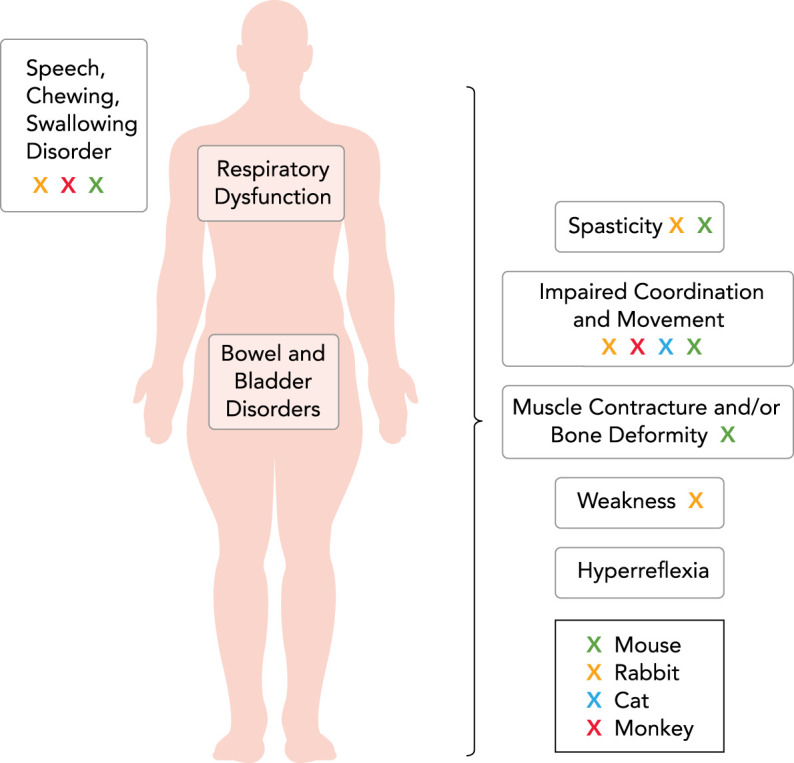
Physical impairments and secondary disorders associated with spastic cerebral palsy in humans In addition to spasticity, the essential diagnostic criterion for spastic CP includes impaired movement and/or coordination, which are determined clinically based on developmental norms for acquiring motor skills. In humans, impaired movement includes difficulty achieving motor milestones, crawling, standing, or walking, or difficulty with sitting or postural control. Note that although impaired movement is observed in monkey (red), cat (blue), rabbit (yellow), and mouse (green) models, spasticity is exhibited only in the mouse and rabbit. Neither cardinal symptoms nor signs of spastic CP are observed in any of the hamster, rat, or sheep models. Clearly, animal models that more closely resemble clinical phenotypes are needed for rational approaches to the understanding of the disease mechanisms and eventual translation to treatment.
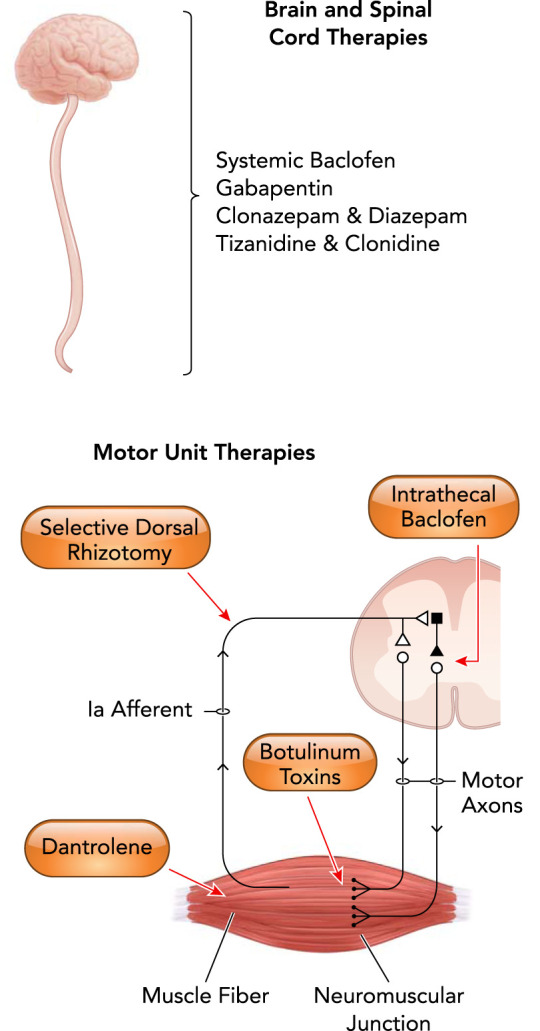
Medical and surgical interventions in the treatment of spastic cerebral palsy All of the current clinical treatments for spastic CP involve both the brain and the spinal cord. Indeed, most treatments exclusively affect the spinal cord, motor neuron and/or motor unit alone. Treatment with baclofen, a presynaptic GABA agonist, may be orally (systemic) or intrathecally (targeting spinal cord neurons) administered. Gabapentin is a mild GABAmimetic and binds the α2δ subunit of voltage-gated Ca2+ channels. Clonazapam and diazepam are similar GABA receptor agonists. Tizanidine and clonidine primarily reduce interneuron activity within the spinal cord via agony of α2 adrenergic receptors. Selective dorsal rhizotomy selectively removes Ia afferent inputs to motor neurons, reducing their reflex excitability. Dantrolene works at the level of skeletal muscle, inhibiting the release of Ca2+ from the sarcoplasmic reticulum.
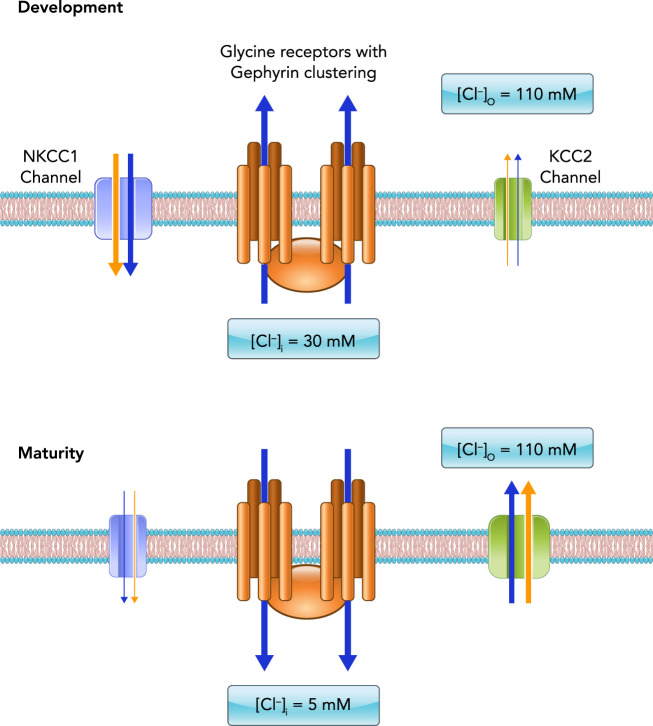
Maturation of inhibitory neurotransmission is dependent on chloride channel expression During development, the opening of ionotropic chloride channels due to GABAergic or glycinergic receptor activation (glycine receptor pentamers with gephyrin clustering shown in orange) leads to chloride efflux (blue arrows) from the neuron, depolarizing the membrane (black bilayer). This is due to high intracellular chloride concentrations (~30 mM) engendered by the abundant expression of NKCC1 chloride transporter (teal) and low expression of the KCC2 chloride transporter (green). The relative expression of these transporters reverses during later postnatal neuronal maturation, such that KCC2 becomes much more abundant and NKCC1 expression is negligible. As a result, internal chloride concentrations in mature neurons is much lower (~5 mM), such that GABAergic or glycinergic receptor activation leads to influx of chloride through ionotropic channels and the hyperpolarization of the membrane. Note that potassium (and sodium in NKCC1) is also co-transported through these channels (yellow arrows).
References
-
- Anstee QM, Knapp S, Maguire EP, Hosie AM, Thomas P, Mortensen M, Bhome R, Martinez A, Walker SE, Dixon CI, Ruparelia K, Montagnese S, Kuo YT, Herlihy A, Bell JD, Robinson I, Guerrini I, McQuillin A, Fisher EM, Ungless MA, Gurling HM, Morgan MY, Brown SD, Stephens DN, Belelli D, Lambert JJ, Smart TG, Thomas HC. Mutations in the Gabrb1 gene promote alcohol consumption through increased tonic inhibition. Nat Commun 4: 2816, 2013. doi:10.1038/ncomms3816. - DOI - PMC - PubMed
-
- Arneson CL, Durkin MS, Benedict RE, Kirby RS, Yeargin-Allsopp M, Van Naarden Braun K, Doernberg NS. Prevalence of cerebral palsy: Autism and Developmental Disabilities Monitoring Network, three sites, United States, 2004. Disabil Health J 2: 45–48, 2009. doi:10.1016/j.dhjo.2008.08.001. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous