

Position statement for the diagnosis and management of anogenital warts
- PMID: 30968980
- PMCID: PMC6593709
- DOI: 10.1111/jdv.15570
Position statement for the diagnosis and management of anogenital warts
Abstract
Background: Anogenital warts (AGW) can cause economic burden on healthcare systems and are associated with emotional, psychological and physical issues.
Objective: To provide guidance to physicians on the diagnosis and management of AGW.
Methods: Fourteen global experts on AGW developed guidance on the diagnosis and management of AGW in an effort to unify international recommendations. Guidance was developed based on published international and national AGW guidelines and an evaluation of relevant literature published up to August 2016. Authors provided expert opinion based on their clinical experiences.
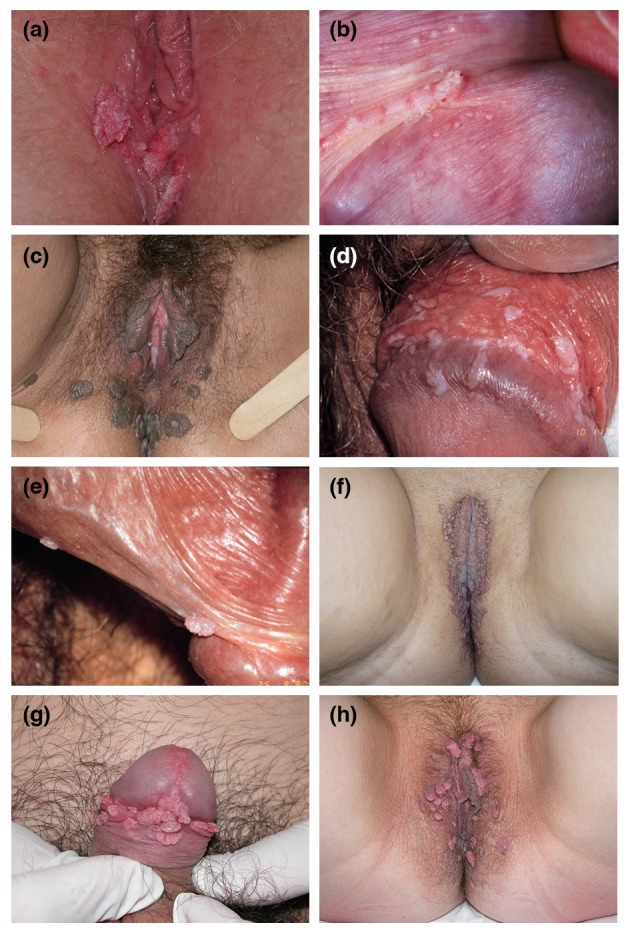
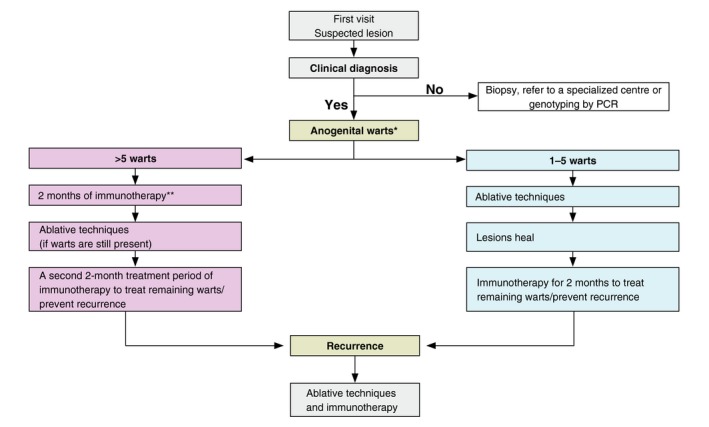
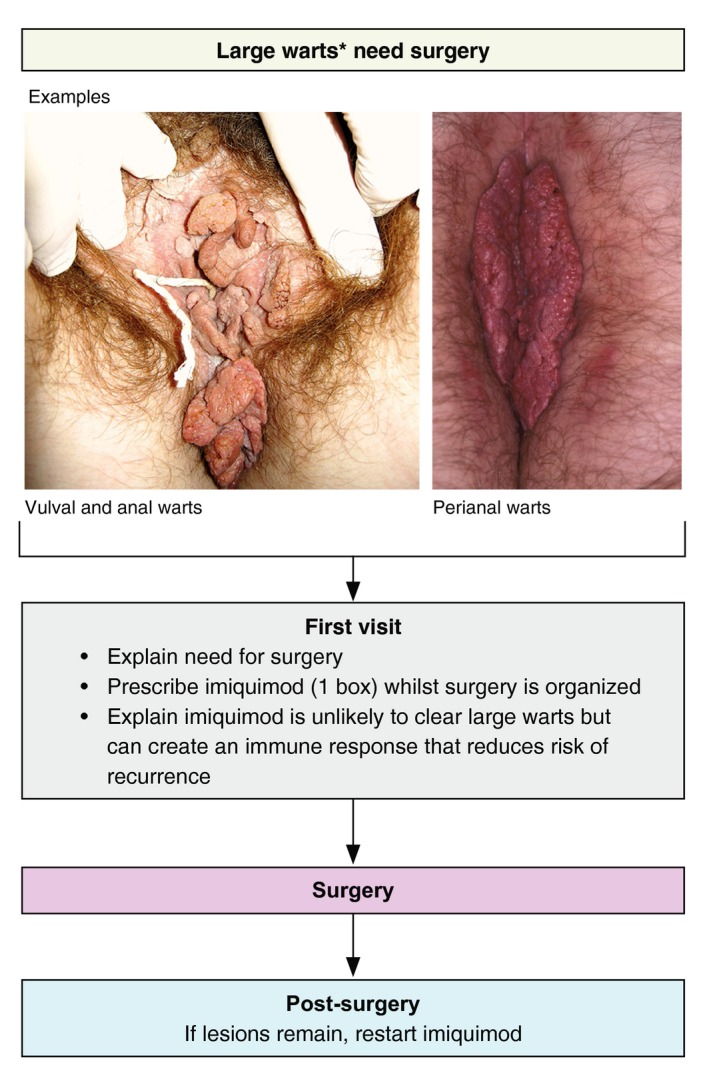
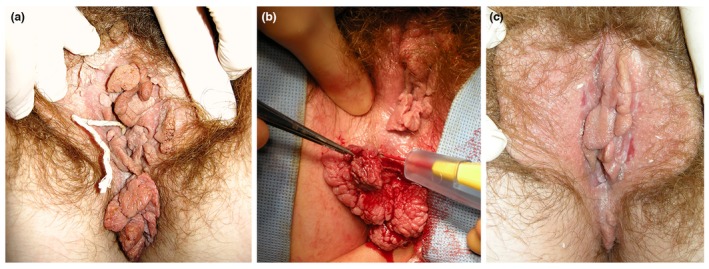
Results: A checklist for a patient's initial consultation is provided to help physicians when diagnosing AGW to get the relevant information from the patient in order to manage and treat the AGW effectively. A number of frequently asked questions are also provided to aid physicians when communicating with patients about AGW. Treatment of AGW should be individualized and selected based on the number, size, morphology, location, and keratinization of warts, and whether they are new or recurrent. Different techniques can be used to treat AGW including ablation, immunotherapy and other topical therapies. Combinations of these techniques are thought to be more effective at reducing AGW recurrence than monotherapy. A simplified algorithm was created suggesting patients with 1-5 warts should be treated with ablation followed by immunotherapy. Patients with >5 warts should use immunotherapy for 2 months followed by ablation and a second 2-month course of immunotherapy. Guidance for daily practice situations and the subsequent action that can be taken, as well as an algorithm for treatment of large warts, were also created.
Conclusion: The guidance provided will help physicians with the diagnosis and management of AGW in order to improve the health and quality of life of patients with AGW.
© 2019 The Authors Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures



References
-
- Lynde C, Vender R, Bourcier M et al Clinical features of external genital warts. J Cutan Med Surg 2013; 17(Suppl 2): S55–S60. - PubMed
-
- Bhatia N, Lynde C, Vender R et al Understanding genital warts: epidemiology, pathogenesis, and burden of disease of human papillomavirus. J Cutan Med Surg 2013; 17(Suppl 2): S47–S54. - PubMed
-
- Goon P, Sonnex C. Frequently asked questions about genital warts in the genitourinary medicine clinic: an update and review of recent literature. Sex Transm Infect 2008; 84: 3–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
