

Influence of New Technologies on Post-Stroke Rehabilitation: A Comparison of Armeo Spring to the Kinect System
- PMID: 30970655
- PMCID: PMC6524064
- DOI: 10.3390/medicina55040098
Influence of New Technologies on Post-Stroke Rehabilitation: A Comparison of Armeo Spring to the Kinect System
Abstract
Background: New technologies to improve post-stroke rehabilitation outcomes are of great interest and have a positive impact on functional, motor, and cognitive recovery. Identifying the most effective rehabilitation intervention is a recognized priority for stroke research and provides an opportunity to achieve a more desirable effect.
Objective: The objective is to verify the effect of new technologies on motor outcomes of the upper limbs, functional state, and cognitive functions in post-stroke rehabilitation.
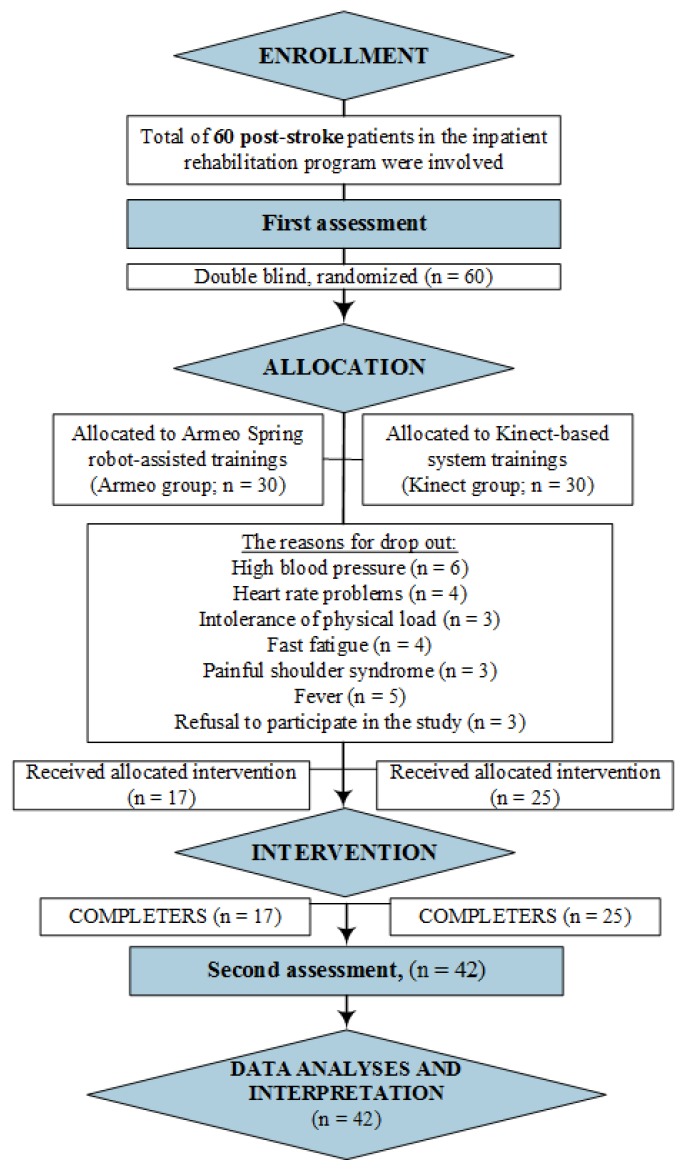
Methods: Forty two post-stroke patients (8.69 ± 4.27 weeks after stroke onset) were involved in the experimental study during inpatient rehabilitation. Patients were randomly divided into two groups: conventional programs were combined with the Armeo Spring robot-assisted trainer (Armeo group; n = 17) and the Kinect-based system (Kinect group; n = 25). The duration of sessions with the new technological devices was 45 min/day (10 sessions in total). Functional recovery was compared among groups using the Functional Independence Measure (FIM), and upper limbs' motor function recovery was compared using the Fugl⁻Meyer Assessment Upper Extremity (FMA-UE), Modified Ashworth Scale (MAS), Hand grip strength (dynamometry), Hand Tapping test (HTT), Box and Block Test (BBT), and kinematic measures (active Range Of Motion (ROM)), while cognitive functions were assessed by the MMSE (Mini-Mental State Examination), ACE-R (Addenbrooke's Cognitive Examination-Revised), and HAD (Hospital Anxiety and Depression Scale) scores.
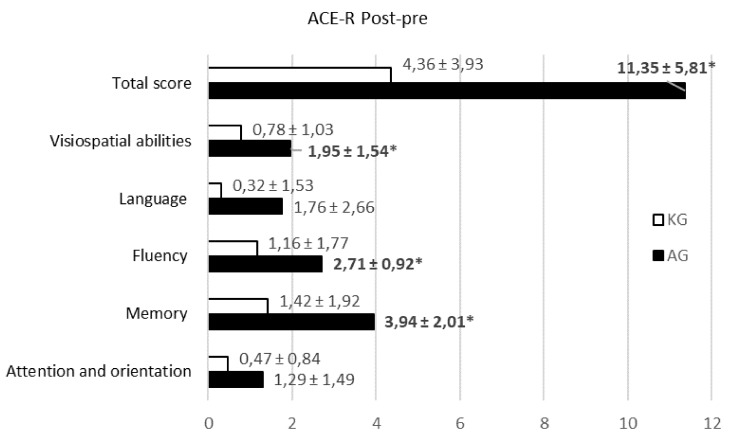
Results: Functional independence did not show meaningful differences in scores between technologies (p > 0.05), though abilities of self-care were significantly higher after Kinect-based training (p < 0.05). The upper limbs' kinematics demonstrated higher functional recovery after robot training: decreased muscle tone, improved shoulder and elbow ROMs, hand dexterity, and grip strength (p < 0.05). Besides, virtual reality games involve more arm rotation and performing wider movements. Both new technologies caused an increase in overall global cognitive changes, but visual constructive abilities (attention, memory, visuospatial abilities, and complex commands) were statistically higher after robotic therapy. Furthermore, decreased anxiety level was observed after virtual reality therapy (p < 0.05).
Conclusions: Our study displays that even a short-term, two-week training program with new technologies had a positive effect and significantly recovered post-strokes functional level in self-care, upper limb motor ability (dexterity and movements, grip strength, kinematic data), visual constructive abilities (attention, memory, visuospatial abilities, and complex commands) and decreased anxiety level.
Keywords: Armeo; Kinect; cognitive recovery; hand motor function; stroke rehabilitation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Liao W., McCombe Waller S., Whitall J. Kinect-based individualized upper extremity rehabilitation is effective and feasible for individuals with stroke using a transition from clinic to home protocol. Cogent. Med. 2018;5:1–12. doi: 10.1080/2331205X.2018.1428038. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
