

Biomarkers of Dietary Omega-6 Fatty Acids and Incident Cardiovascular Disease and Mortality
- PMID: 30971107
- PMCID: PMC6582360
- DOI: 10.1161/CIRCULATIONAHA.118.038908
Biomarkers of Dietary Omega-6 Fatty Acids and Incident Cardiovascular Disease and Mortality
Abstract
Background: Global dietary recommendations for and cardiovascular effects of linoleic acid, the major dietary omega-6 fatty acid, and its major metabolite, arachidonic acid, remain controversial. To address this uncertainty and inform international recommendations, we evaluated how in vivo circulating and tissue levels of linoleic acid (LA) and arachidonic acid (AA) relate to incident cardiovascular disease (CVD) across multiple international studies.
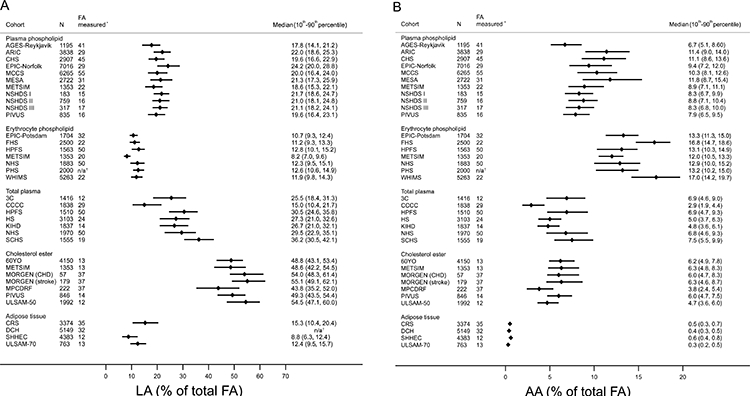
Methods: We performed harmonized, de novo, individual-level analyses in a global consortium of 30 prospective observational studies from 13 countries. Multivariable-adjusted associations of circulating and adipose tissue LA and AA biomarkers with incident total CVD and subtypes (coronary heart disease, ischemic stroke, cardiovascular mortality) were investigated according to a prespecified analytic plan. Levels of LA and AA, measured as the percentage of total fatty acids, were evaluated linearly according to their interquintile range (ie, the range between the midpoint of the first and fifth quintiles), and categorically by quintiles. Study-specific results were pooled using inverse-variance-weighted meta-analysis. Heterogeneity was explored by age, sex, race, diabetes mellitus, statin use, aspirin use, omega-3 levels, and fatty acid desaturase 1 genotype (when available).
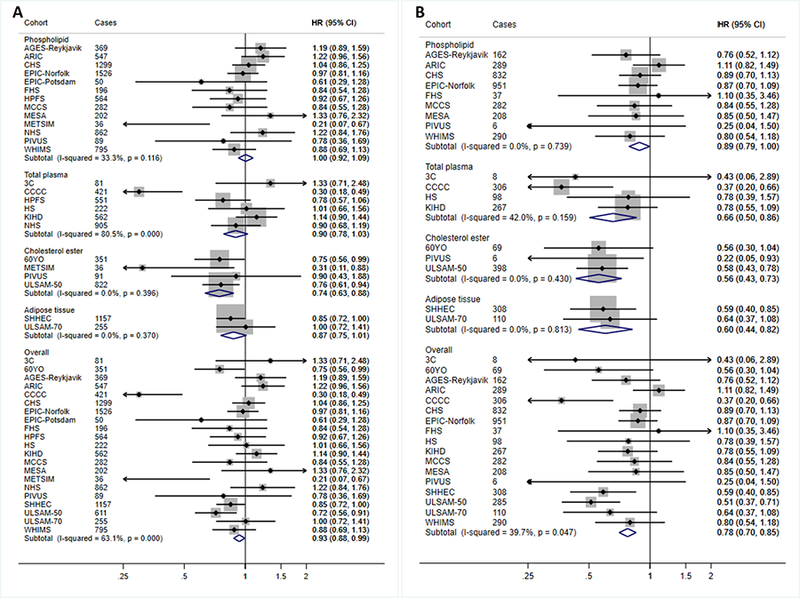
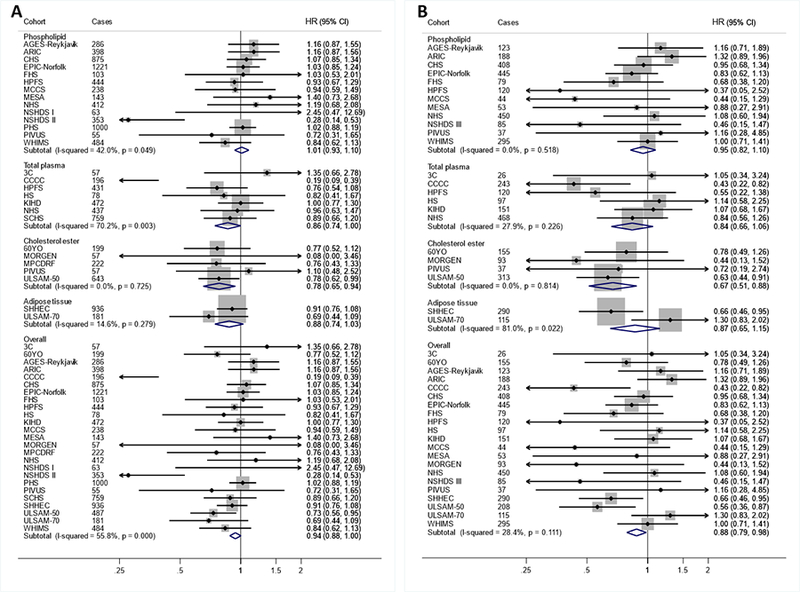
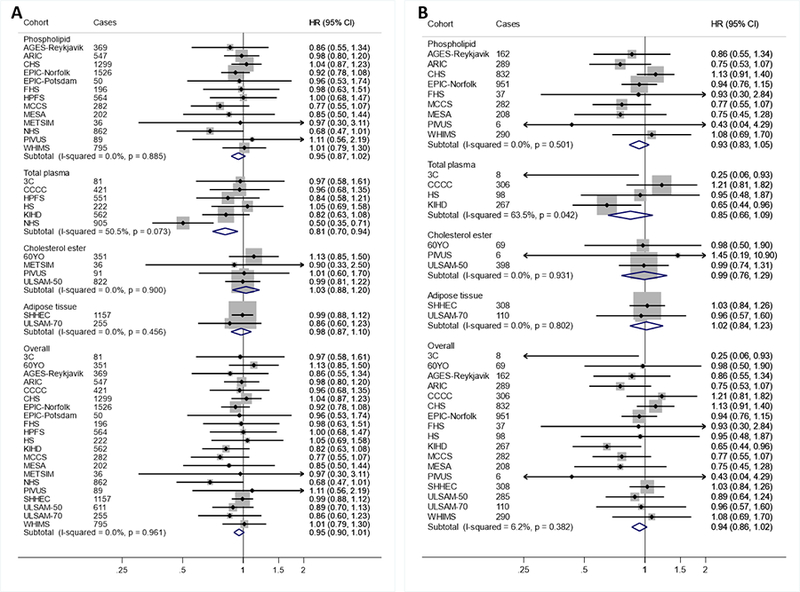
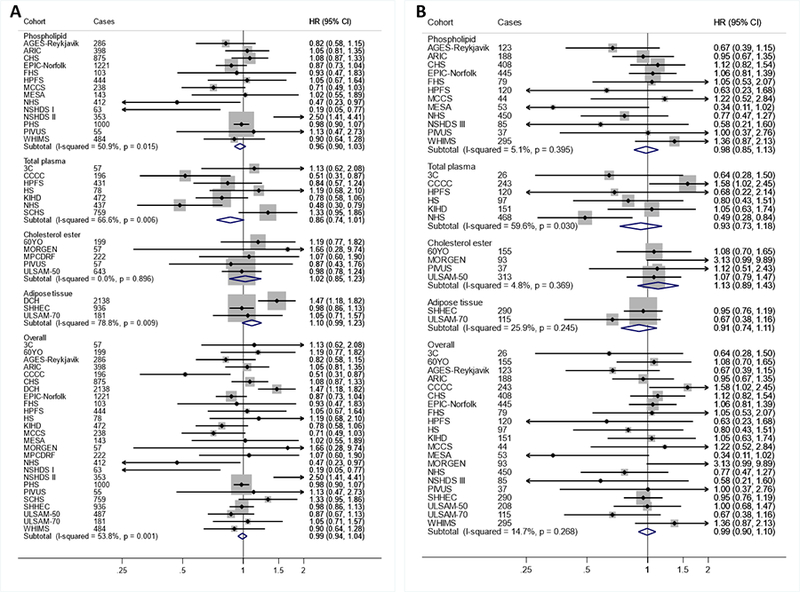
Results: In 30 prospective studies with medians of follow-up ranging 2.5 to 31.9 years, 15 198 incident cardiovascular events occurred among 68 659 participants. Higher levels of LA were significantly associated with lower risks of total CVD, cardiovascular mortality, and ischemic stroke, with hazard ratios per interquintile range of 0.93 (95% CI, 0.88-0.99), 0.78 (0.70-0.85), and 0.88 (0.79-0.98), respectively, and nonsignificantly with lower coronary heart disease risk (0.94; 0.88-1.00). Relationships were similar for LA evaluated across quintiles. AA levels were not associated with higher risk of cardiovascular outcomes; in a comparison of extreme quintiles, higher levels were associated with lower risk of total CVD (0.92; 0.86-0.99). No consistent heterogeneity by population subgroups was identified in the observed relationships.
Conclusions: In pooled global analyses, higher in vivo circulating and tissue levels of LA and possibly AA were associated with lower risk of major cardiovascular events. These results support a favorable role for LA in CVD prevention.
Keywords: arachidonic acid; biomarkers; cardiovascular diseases; diet; epidemiology; linoleic acid; primary prevention.
Conflict of interest statement
DISCLOSURES
Drs. Wu and Micha report research support from Unilever for this work. Dr. Mozaffarian reports research funding from the National Institutes of Health and the Gates Foundation; personal fees from GOED, DSM, Nutrition Impact, Pollock Communications, Bunge, Indigo Agriculture, Amarin, Acasti Pharma, and America’s Test Kitchen; scientific advisory board, Elysium Health (with stock options), Omada Health, and DayTwo; and chapter royalties from UpToDate; all outside the submitted work. Dr. Psaty serves on the DSMB of a clinical trial funded by the manufacturer (Zoll LifeCor) and on the Steering Committee of the Yale Open Data Access Project funded by Johnson & Johnson. No other conflicts were reported.
Figures
Comment in
-
Omega-6 Fatty Acids and Cardiovascular Disease.Circulation. 2019 May 21;139(21):2437-2439. doi: 10.1161/CIRCULATIONAHA.119.040331. Circulation. 2019. PMID: 31107617 No abstract available.
References
-
- Harris WS, Mozaffarian D, Rimm E, Kris-Etherton P, Rudel LL, Appel LJ, Engler MM, Engler MB and Sacks F. Omega-6 Fatty Acids and Risk for Cardiovascular Disease: A Science Advisory From the American Heart Association Nutrition Subcommittee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Cardiovascular Nursing; and Council on Epidemiology and Prevention. Circulation. 2009;119:902–907. - PubMed
-
- Vannice G and Rasmussen H. Position of the Academy of Nutrition and Dietetics: Dietary Fatty Acids for Healthy Adults. J Acad Nutr Diet. 2014;114:136–153. - PubMed
-
- Food and Agriculture Organization of the United Nations. Fats and fatty acids in human nutrition : report of an expert consultation : 10-14 November 2008, Geneva. Rome: Food and Agriculture Organization of the United Nations; 2010.
-
- Legrand P, Morise A and Kalonji E. Update of French nutritional recommendations for fatty acids. World Rev Nutr Diet. 2011;102:137–143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- R01 HL034594/HL/NHLBI NIH HHS/United States
- N01 AG012100/AG/NIA NIH HHS/United States
- R01 HL059367/HL/NHLBI NIH HHS/United States
- MC_UU_12015/1/MRC_/Medical Research Council/United Kingdom
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- R01 HL026490/HL/NHLBI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
- R01 CA097193/CA/NCI NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- R21 HL088081/HL/NHLBI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- BHF_/British Heart Foundation/United Kingdom
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- P01 CA055075/CA/NCI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- R01 CA144034/CA/NCI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- G1000143/MRC_/Medical Research Council/United Kingdom
- N01 HC095166/HC/NHLBI NIH HHS/United States
- U01 HG004402/HG/NHGRI NIH HHS/United States
- ZIA AG007380/ImNIH/Intramural NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- P30 DK046200/DK/NIDDK NIH HHS/United States
- U01 CA182876/CA/NCI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- 14136/CRUK_/Cancer Research UK/United Kingdom
- N01 HC055222/HL/NHLBI NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- G0401527/MRC_/Medical Research Council/United Kingdom
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- R01 HL088521/HL/NHLBI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- R01 AA011181/AA/NIAAA NIH HHS/United States
- R01 CA049449/CA/NCI NIH HHS/United States
- R01 CA040360/CA/NCI NIH HHS/United States
- CSO_/Chief Scientist Office/United Kingdom
- R01 AG023629/AG/NIA NIH HHS/United States
- R01 HL087641/HL/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- MC_UU_12015/5/MRC_/Medical Research Council/United Kingdom
- R01 HL081549/HL/NHLBI NIH HHS/United States
- R01 CA034944/CA/NCI NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- UM1 CA182876/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
