

SponDT (Spondylodiscitis Diagnosis and Treatment): spondylodiscitis scoring system
- PMID: 30971277
- PMCID: PMC6458762
- DOI: 10.1186/s13018-019-1134-9
SponDT (Spondylodiscitis Diagnosis and Treatment): spondylodiscitis scoring system
Abstract
Background: Spondylodiscitis is a chameleon among infectious diseases due to the lack of specific symptoms with which it is associated. It is nevertheless a serious infection, with 7% mortality of hospitalized patients, in large part because of delayed diagnosis. The aim of this study was to develop a diagnosis and course-of-disease index to optimize its treatment.
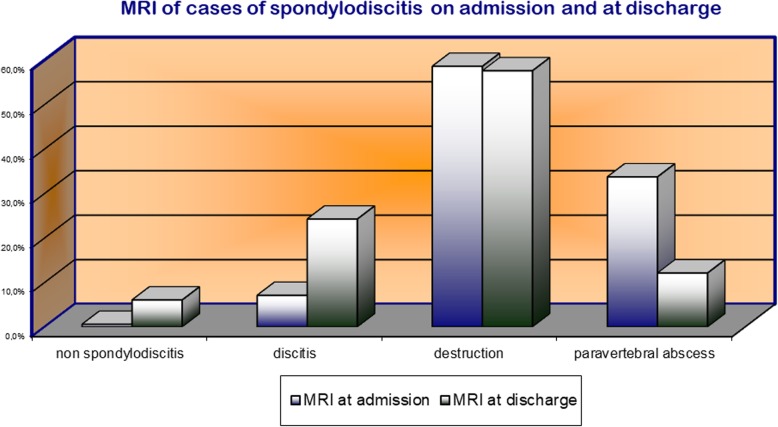
Material and methods: Through analysis of 296 patients between January 1998 and December 2013, we developed a scoring system for spondylodiscitis, which we term SponDT (Spondylodiscitis Diagnosis and Treatment) based on three traits: (1) the inflammatory marker C-reactive protein (CRP) (mg/dl), (2) pain according to a numeric rating scale (NRS) and (3) magnetic resonance imaging (MRI), to monitor its progression following treatment.
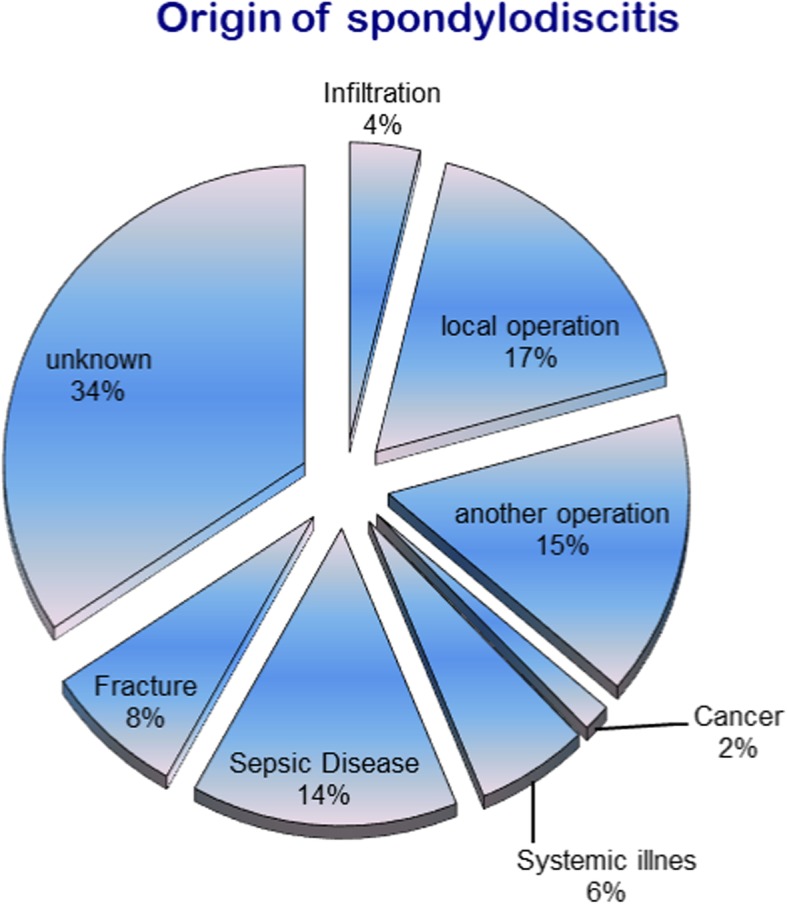
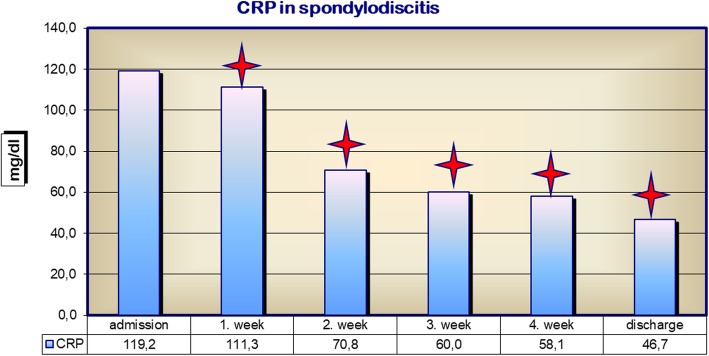
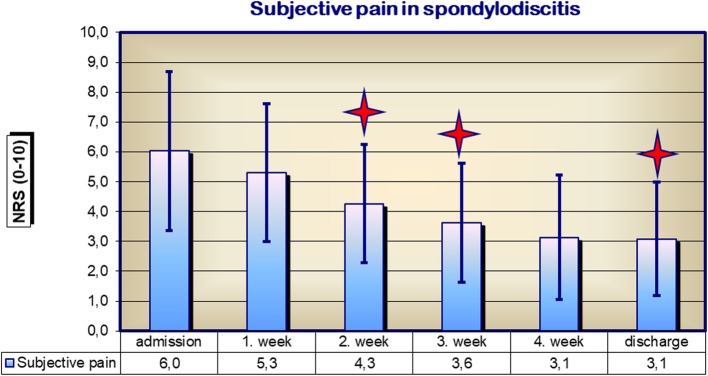
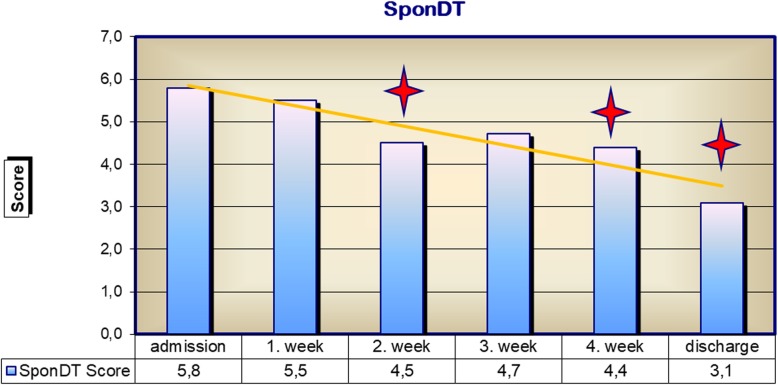
Results: The number of patients receiving treatment increased over the past 15 years of our study. We also found an increasing age of patients at the point of diagnosis across the study, with an average age of 67.7 years. In 34% of patients, spondylodiscitis developed spontaneously. Almost 70% of them did not receive treatment until the first diagnosis using SponDT. Following treatment against spondylodiscitis, pain intensity decreased from 6.0 to 3.1 NRS. The inflammatory markers also decreased (CRP from 119.2 to 46.7 mg/dl). Similarly, MRI revealed a regression in inflammation following treatment. By employing SponDT, patients were diagnosed and entered into treatment with a score of 5.6 (severe spondylodiscitis) and discharged with a score of 2.4 (light/healed spondylodiscitis).
Conclusion: SponDT can be used to support the diagnosis of spondylodiscitis, particularly in patients suffering from back pain and elevated levels of inflammation, and can be used during the course of treatment to optimize control of therapy.
Level of evidence: IIa-evidence from at least one well-designed controlled trial which is not randomized.
Keywords: Classification of severity; Scoring system; Spondylodiscitis.
Conflict of interest statement
Authors’ information
Not applicable
Ethics approval and consent to participate
Ethical approval for these studies has been granted by the University of Jena, Germany. All procedures were in accordance with the ethical standards of the institutional research committee. The participants declared their consent in writing.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mückley T, Kirschner M, HierholzerC HGO. Spondylitis – Spondylodiszitis: neue Therapiekonzepte. Trauma Berufskrankh. 2003;5(suppl 2):296–304. doi: 10.1007/s10039-002-0660-5. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
