

A Cohort Study of the Impact of Carbapenem-Resistant Enterobacteriaceae Infections on Mortality of Patients Presenting with Sepsis
- PMID: 30971443
- PMCID: PMC6458433
- DOI: 10.1128/mSphere.00052-19
A Cohort Study of the Impact of Carbapenem-Resistant Enterobacteriaceae Infections on Mortality of Patients Presenting with Sepsis
Abstract
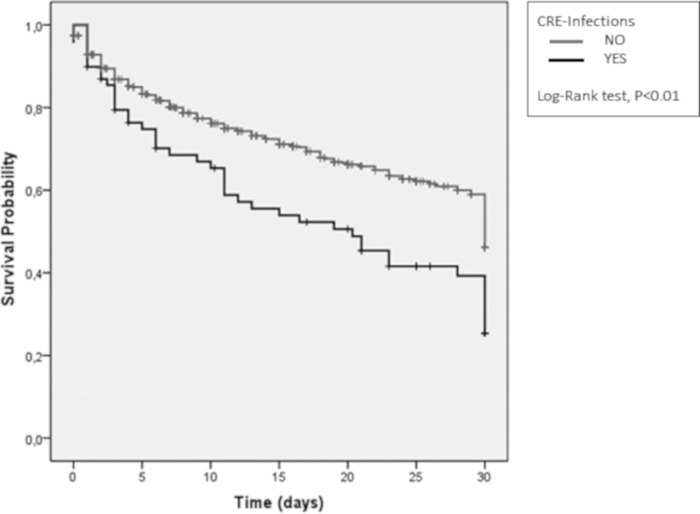
The objective of this study is to evaluate the impact of carbapenem-resistant Enterobacteriaceae (CRE) infection on sepsis 30-day mortality. A retrospective cohort of patients >18 years old with sepsis and organ dysfunction or septic shock was conducted. Univariate analysis was done for variables potentially related to 30-day mortality, and the ones with P values of <0.05 were included in a backward stepwise hierarchic Cox regression model. Variables that remained with P values of <0.05 were retained in the model. A total of 1,190 sepsis episodes were analyzed. Gram-negative bacterial infections occurred in 391 (68.5%) of 571 patients with positive cultures, of which 69 (17.7%) were caused by a CRE organism. Patients with CRE infections had significantly higher 30-day mortality: 63.8% versus 33.4% (P < 0.01). CRE infection was also associated with a lower rate of appropriate empirical therapy (P < 0.01) and with the presence of septic shock (P < 0.01). In the hierarchic multivariate model, CRE remained significant when controlling for demographic variables, comorbidities, and infection site but lost significance when controlling for septic shock and appropriate empirical therapy. Older age (P < 0.01), HIV-positive status (P < 0.01), cirrhosis (P < 0.01), septic shock (P < 0.01), higher quick sepsis-related organ failure assessment (quick-SOFA) (P < 0.01), and appropriate empirical therapy (P = 0.01) remained in the final model. CRE infections were associated with higher crude mortality rates. A lower rate of appropriate empirical therapy and late diagnosis were more frequent in this group, and improvement of stewardship programs is needed.IMPORTANCE The importance of this work relies on exploring the impact of multidrug-resistant bacterial infections such as those with carbapenem-resistant Enterobacteriaceae (CRE) on sepsis mortality. These infections are growing at alarming rates worldwide and are now among the most frequent and difficult-to-treat bacteria due to the very few options for susceptible antimicrobials available. This study examined 1,190 sepsis episodes, and the main findings were as follows: (i) the prevalence of CRE infections significantly increased over time, (ii) CRE infection was associated with higher 30-day mortality than that of patients with other infections (63.8% versus 33.4%), and (iii) the effect of CRE on mortality was probably influenced by the fact that those patients received lower rates of empirical therapy with active antibiotics and were also diagnosed in more advanced stages of sepsis (septic shock). Those findings point to the need for rapid diagnostic methods to identify these bacteria and the need to adjust therapeutic guidelines to this worrisome epidemiological scenario.
Keywords: Gram-negative bacteria; carbapenem resistant; mortality; sepsis; septic shock.
Copyright © 2019 Sabino et al.
Figures
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP. 2017. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Bassetti M, Giacobbe DR, Giamarellou H, Viscoli C, Daikos GL, Dimopoulos G, De Rosa FG, Giamarellos-Bourboulis EJ, Rossolini GM, Righi E, Karaiskos I, Tumbarello M, Nicolau DP, Viale PL, Poulakou G. 2018. Management of KPC-producing Klebsiella pneumoniae infections. Clin Microbiol Infect 24:133–144. doi: 10.1016/j.cmi.2017.08.030. - DOI - PubMed
-
- Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. 2017. Carbapenem resistance, inappropriate empiric treatment and outcomes among patients hospitalized with Enterobacteriaceae urinary tract infection, pneumonia and sepsis. BMC Infect Dis 17:279. doi: 10.1186/s12879-017-2383-z. - DOI - PMC - PubMed
-
- Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, Cormican M, Cornaglia G, Garau J, Gniadkowski M, Hayden MK, Kumarasamy K, Livermore DM, Maya JJ, Nordmann P, Patel JB, Paterson DL, Pitout J, Villegas MV, Wang H, Woodford N, Quinn JP. 2013. Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. Lancet Infect Dis 13:785–796. doi: 10.1016/S1473-3099(13)70190-7. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
