

The Coincidence Between Increasing Age, Immunosuppression, and the Incidence of Patients With Glioblastoma
- PMID: 30971917
- PMCID: PMC6446059
- DOI: 10.3389/fphar.2019.00200
The Coincidence Between Increasing Age, Immunosuppression, and the Incidence of Patients With Glioblastoma
Abstract
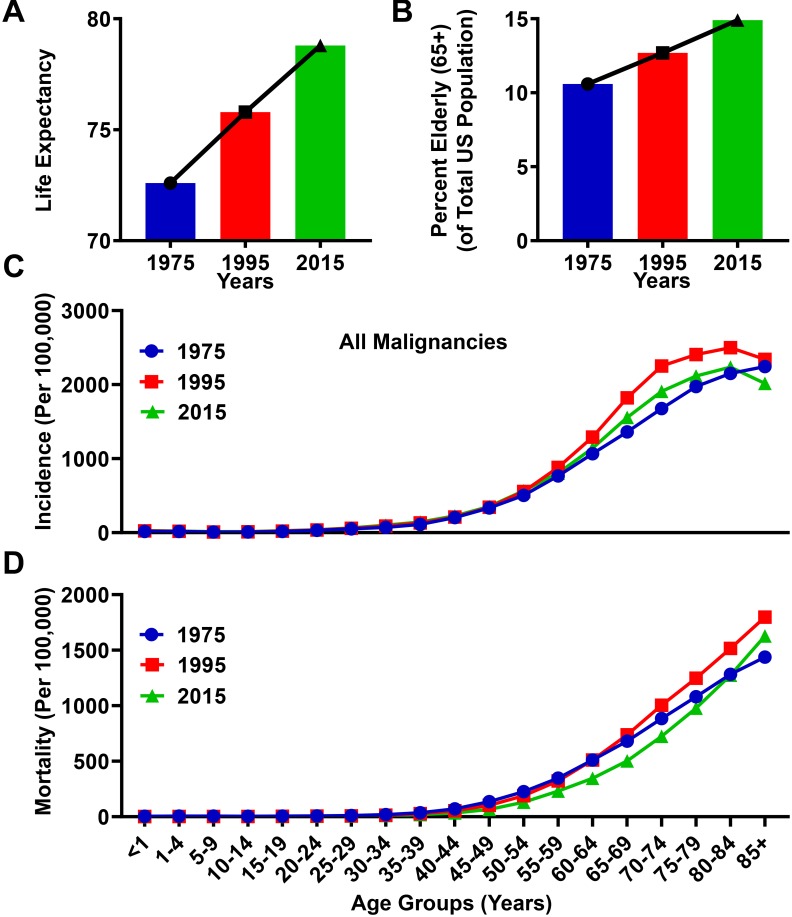
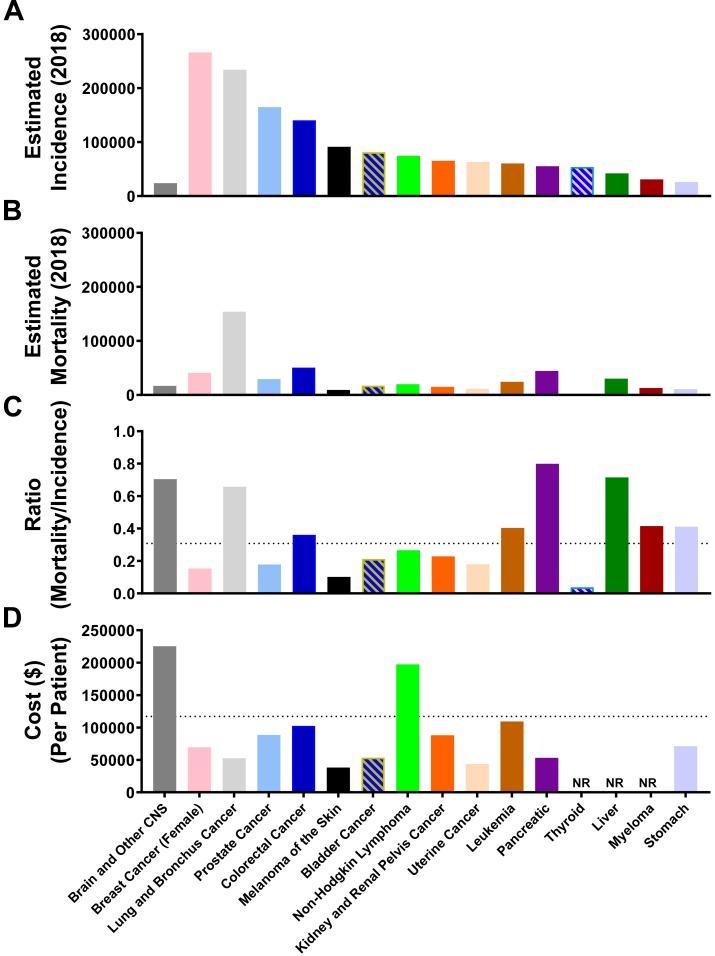
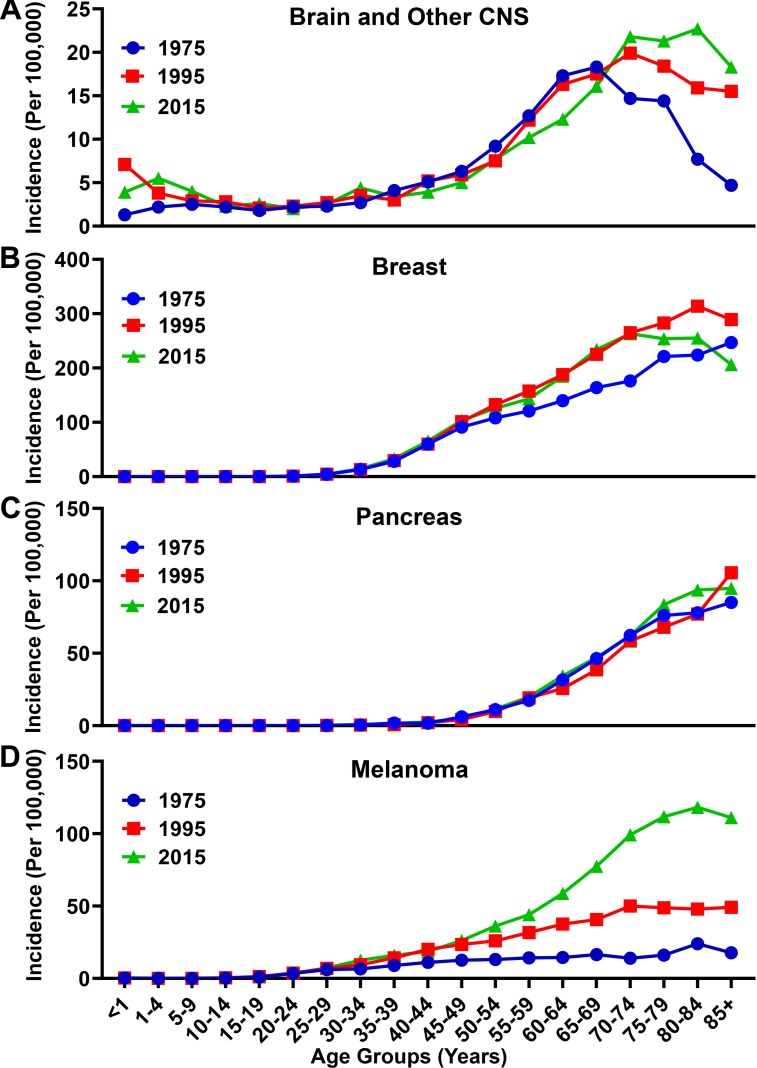
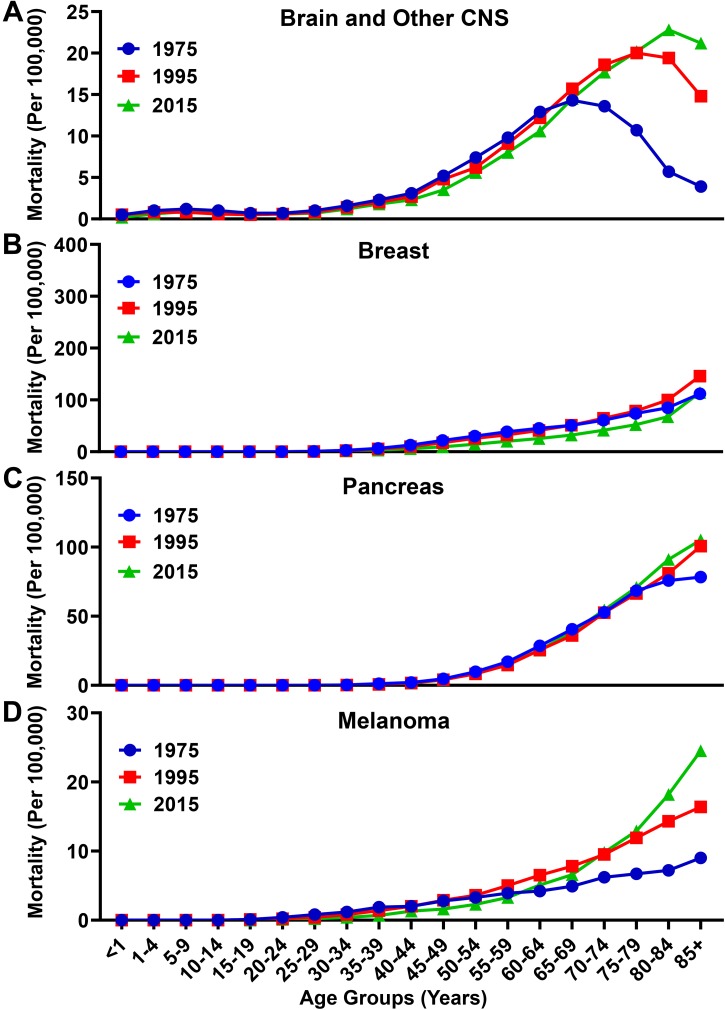
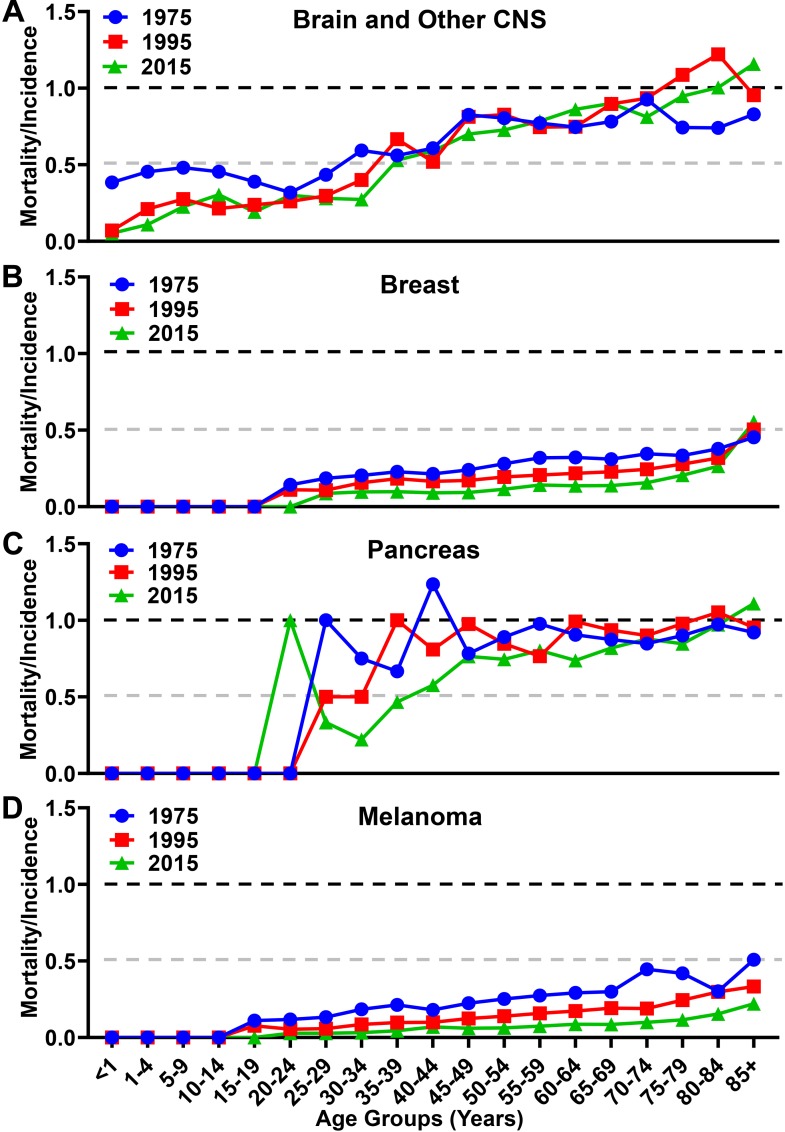
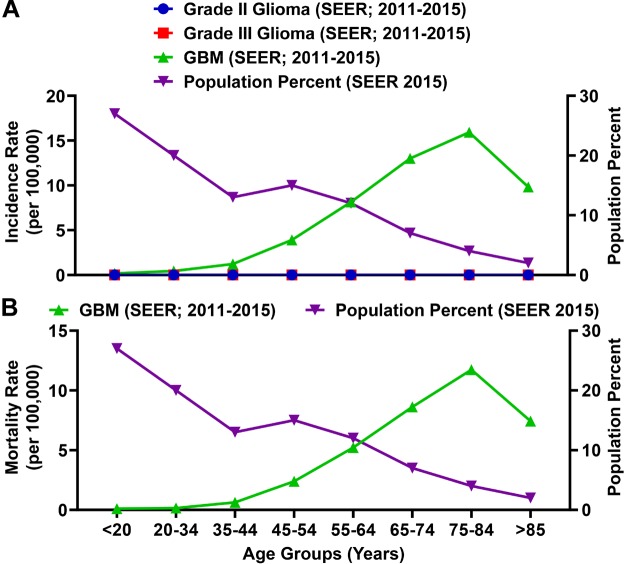
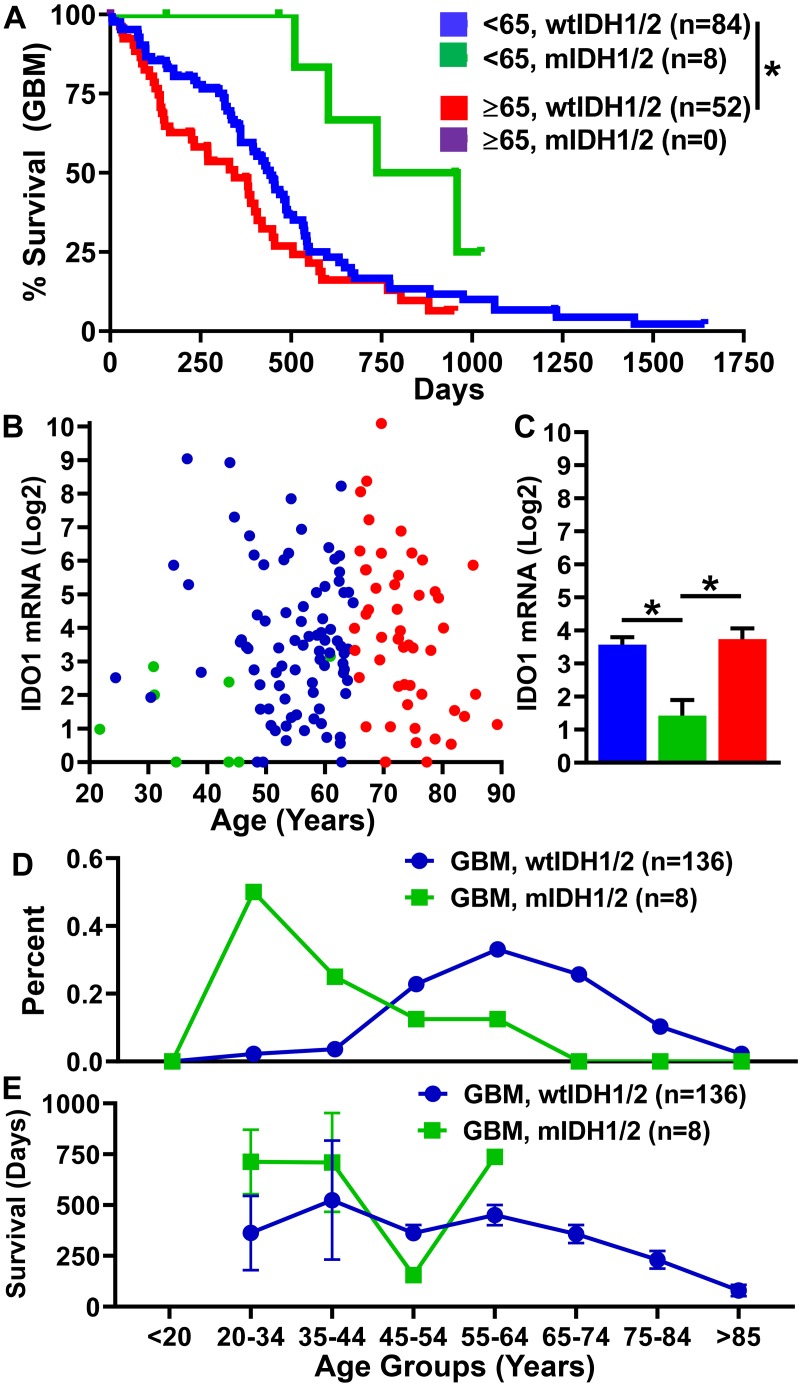
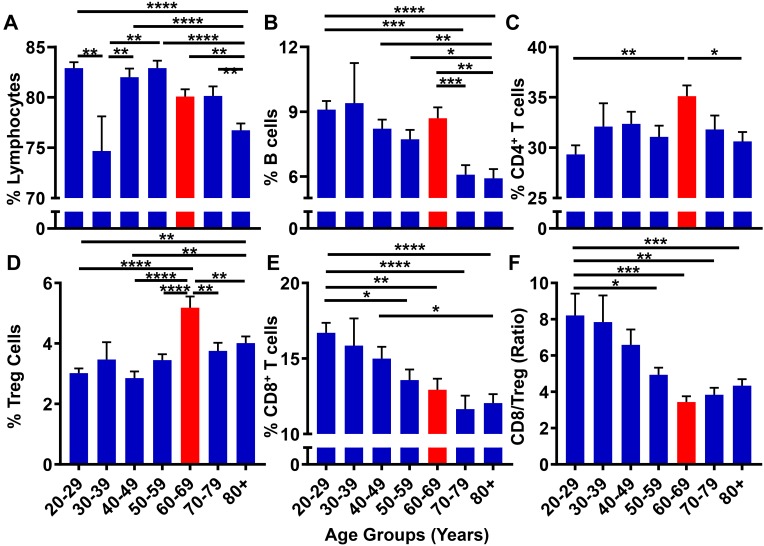
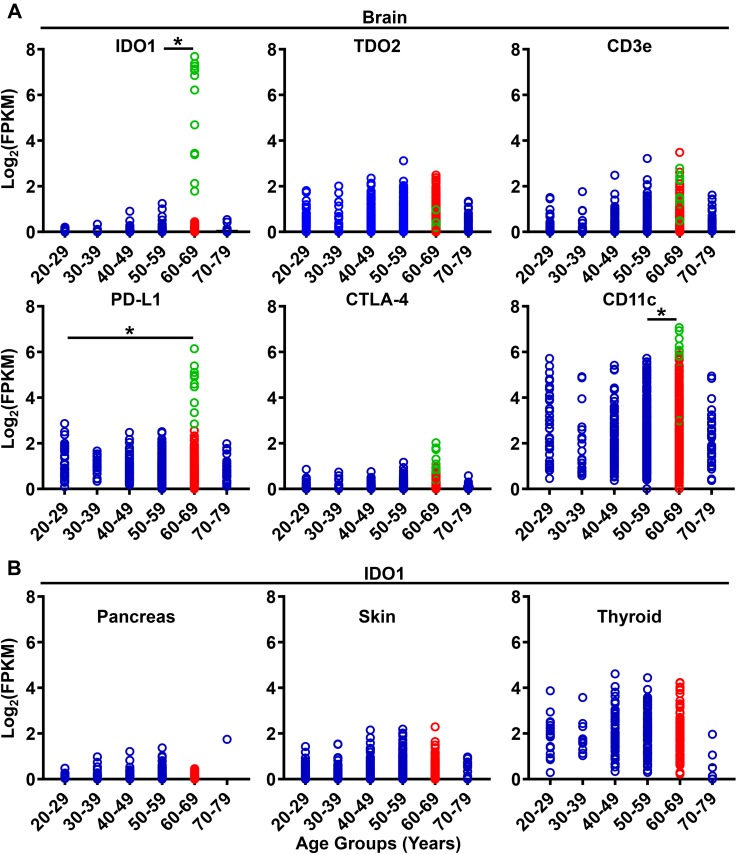
Background: Glioblastoma (GBM) is the most aggressive primary brain tumor in adults and is associated with a median overall survival (mOS) of 16-21 months. Our previous work found a negative association between advanced aging and the survival benefit after treatment with immunotherapy in an experimental brain tumor model. Given the recent phase III clinical success of immunotherapy in patients with many types of cancer, but not for patients with GBM, we hypothesize that aging enhances immunosuppression in the brain and contributes to the lack of efficacy for immunotherapy to improve mOS in patients with malignant glioma. Herein, we compare epidemiological data for the incidence and mortality of patients with central nervous system (CNS) cancers, in addition to immune-related gene expression in the normal human brain, as well as peripheral blood immunological changes across the adult lifespan. Methods: Data were extracted from the National Cancer Institute's surveillance, epidemiology, and end results (SEER)-, the Broad Institute's Genotype Tissue Expression project (GTEx)-, and the University of California San Francisco's 10k Immunomes-databases and analyzed for associations with aging. Results: The proportion of elderly individuals, defined as ≥65 years of age, has predominantly increased for more than 100 years in the United States. Over time, the rise in elderly United States citizens has correlated with an increased incidence and mortality rate associated with primary brain and other CNS cancer. With advanced aging, human mRNA expression for factors associated with immunoregulation including immunosuppressive indoleamine 2,3 dioxygenase 1 (IDO) and programmed death-ligand 1 (PD-L1), as well as the dendritic cell surface marker, CD11c, increase in the brain of normal human subjects, coincident with increased circulating immunosuppressive Tregs and decreased cytolytic CD8+ T cells in the peripheral blood. Strikingly, these changes are maximally pronounced in the 60-69 year old group; consistent with the median age of a diagnosis for GBM. Conclusion: These data demonstrate a significant association between normal human aging and increased immunosuppression in the circulation and CNS; particularly late in life. Our data raise several hypotheses including that, aging: (i) progressively suppresses normal immunosurveillance and thereby contributes to GBM cell initiation and/or outgrowth; (ii) decreases immunotherapeutic efficacy against malignant glioma.
Keywords: IDH; IDO; PD-L1; Treg; aging; biomarker; immunosuppression; immunotherapy.
Figures
References
-
- Antonia S. J., Lopez Martin J. A., Bendell J., Ott P. A., Taylor M., Eder J. P., et al. (2016). Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol. 17 883–895. 10.1016/S1470-2045(16)30098-5 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials