

Exploring the Feasibility of Pipeline Embolization Device Compared With Stent-Assisted Coiling to Treat Non-saccular, Unruptured, Intradural Vertebral Artery Aneurysms
- PMID: 30972007
- PMCID: PMC6443633
- DOI: 10.3389/fneur.2019.00275
Exploring the Feasibility of Pipeline Embolization Device Compared With Stent-Assisted Coiling to Treat Non-saccular, Unruptured, Intradural Vertebral Artery Aneurysms
Abstract
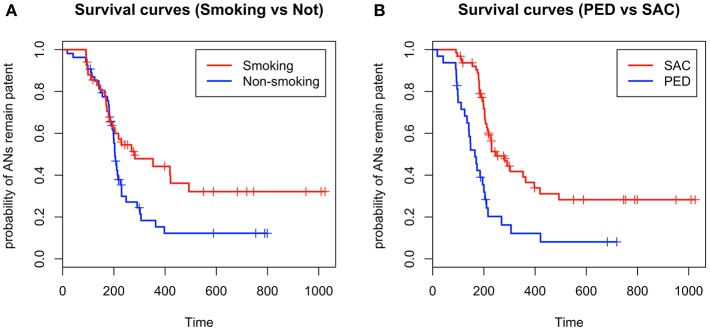
Object: The pipeline embolization device (PED) has been used to treat non-saccular, unruptured, intradural vertebral artery aneurysms at some institutions. However, there is an absence of large controlled studies validating the feasibility of this treatment. This study aimed to explore the therapeutic feasibility of PED by comparing PED treatment with controlled stent-assisted coiling (SAC). Materials and Methods: Thirty-two PED procedures were matched in a 1:2 manner with 64 SAC procedures based on patient age, sex, aneurysm size, and aneurysm location. Technical factors, procedural complications, angiographic results, and clinical outcomes were analyzed and compared. Results: There was no statistically significant difference in technical factors and procedural complications between the two groups (PED vs. SAC, 9.4 vs. 4.7%, P = 0.397). In multivariate analysis, smoking and therapeutic modality were identified as independent predictors of occlusion. Smoking was a risk factor for aneurysm obliteration [hazard ratio (HR) 0.53; 95% confidence interval (CI), 0.31-0.89; P = 0.018]. Aneurysms treated with PED were more likely to achieve obliteration over time compared with aneurysms treated with SAC (HR 2.97; 95% CI, 1.79-4.93; P < 0.001). The rate of favorable clinical outcomes (modified Rankin Scale (mRS), 0-2) was similar between the two groups (PED vs. SAC, 100 vs. 96.9%, P = 0.551). In the SAC group, one patient had neurological deficit with an mRS of four at the latest follow-up. There was no mortality in either group. Conclusions: The PED and SAC groups showed similar technical factors, procedural complications, angiographic results, and favorable clinical outcomes. Aneurysms treated with PED were more prone to obliteration over time than aneurysms treated with SAC. These outcomes suggest, based on short-term follow-up, PED is a safe and feasible strategy for the treatment of non-saccular, unruptured, intradural vertebral artery aneurysms.
Keywords: non-saccular aneurysm; pipeline embolization device; posterior circulation; stent-assisted coiling; vertebral artery aneurysm.
Figures
References
LinkOut - more resources
Full Text Sources