

Clinical implementation of respiratory-gated spot-scanning proton therapy: An efficiency analysis of active motion management
- PMID: 30972922
- PMCID: PMC6523004
- DOI: 10.1002/acm2.12584
Clinical implementation of respiratory-gated spot-scanning proton therapy: An efficiency analysis of active motion management
Abstract
Purpose: The aim of this work is to describe the clinical implementation of respiratory-gated spot-scanning proton therapy (SSPT) for the treatment of thoracic and abdominal moving targets. The experience of our institution is summarized, from initial acceptance and commissioning tests to the development of standard clinical operating procedures for simulation, motion assessment, motion mitigation, treatment planning, and gated SSPT treatment delivery.
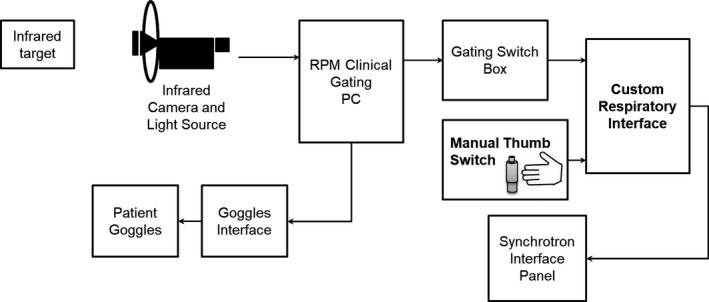
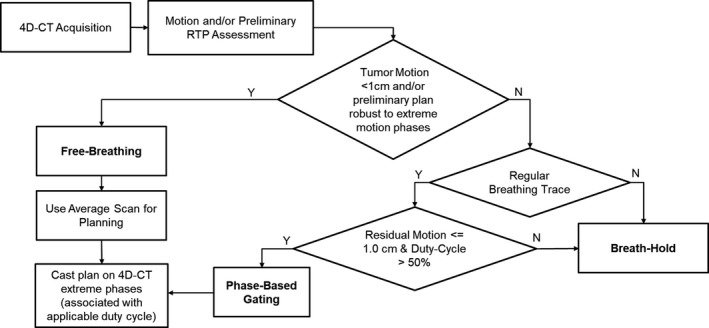
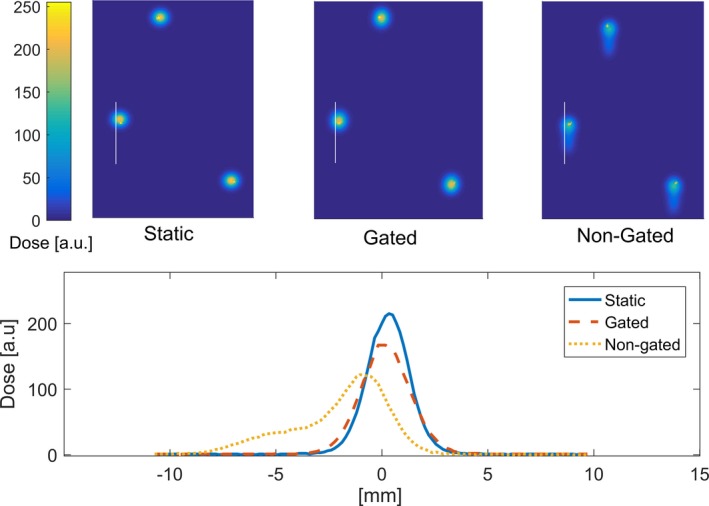
Materials and methods: A custom respiratory gating interface incorporating the Real-Time Position Management System (RPM, Varian Medical Systems, Inc., Palo Alto, CA, USA) was developed in-house for our synchrotron-based delivery system. To assess gating performance, a motion phantom and radiochromic films were used to compare gated vs nongated delivery. Site-specific treatment planning protocols and conservative motion cutoffs were developed, allowing for free-breathing (FB), breath-holding (BH), or phase-gating (Ph-G). Room usage efficiency of BH and Ph-G treatments was retrospectively evaluated using beam delivery data retrieved from our record and verify system and DICOM files from patient-specific quality assurance (QA) procedures.
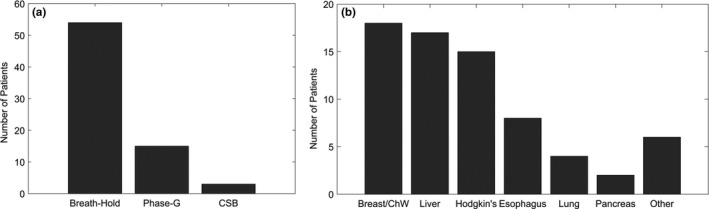
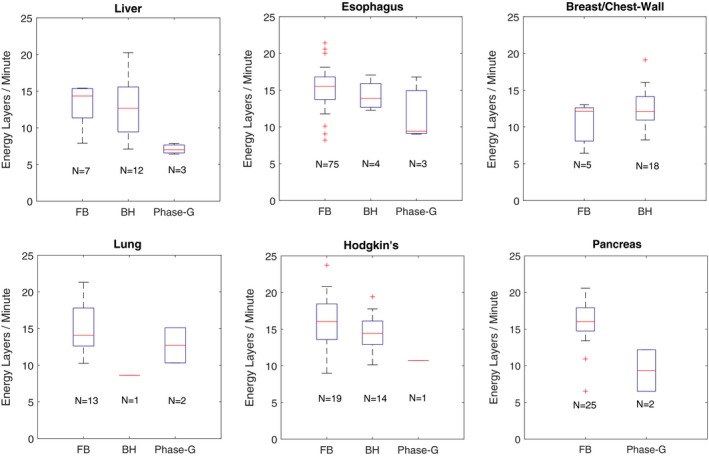
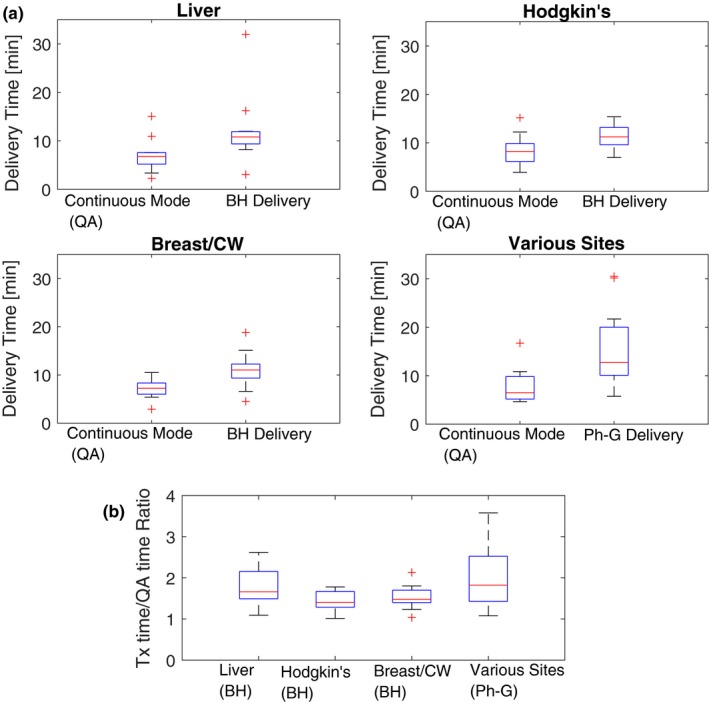
Results: More than 70 patients were treated using active motion management between the launch of our motion mitigation program in October 2015 and the end date of data collection of this study in January 2018. During acceptance procedures, we found that overall system latency is clinically-suitable for Ph-G. Regarding room usage efficiency, the average number of energy layers delivered per minute was <10 for Ph-G, 10-15 for BH and ≥15 for FB, making Ph-G the slowest treatment modality. When comparing to continuous delivery measured during pretreatment QA procedures, the median values of BH treatment time were extended from 6.6 to 9.3 min (+48%). Ph-G treatments were extended from 7.3 to 13.0 min (+82%).
Conclusions: Active motion management has been crucial to the overall success of our SSPT program. Nevertheless, our conservative approach has come with an efficiency cost that is more noticeable in Ph-G treatments and should be considered in decision-making.
Keywords: breath-holding; motion management; phase-gating; proton therapy; spot-scanning.
© 2019 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflicts of interest to disclose. No external funding was received.
Figures
References
-
- Lambert J, Suchowerska N, McKenzie DR, Jackson M. Intrafractional motion during proton beam scanning. Phys Med Biol. 2005;50:4853–4862. - PubMed
-
- Seco J, Robertson D, Trofimov A, Paganetti H. Breathing interplay effects during proton beam scanning: simulation and statistical analysis. Phys Med Biol. 2009;54:N283–N294. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
