

Extracorporeal membrane oxygenation use in the first 24 hours following pediatric heart transplantation: Incidence, risk factors, and outcomes
- PMID: 30973190
- PMCID: PMC6548572
- DOI: 10.1111/petr.13414
Extracorporeal membrane oxygenation use in the first 24 hours following pediatric heart transplantation: Incidence, risk factors, and outcomes
Abstract
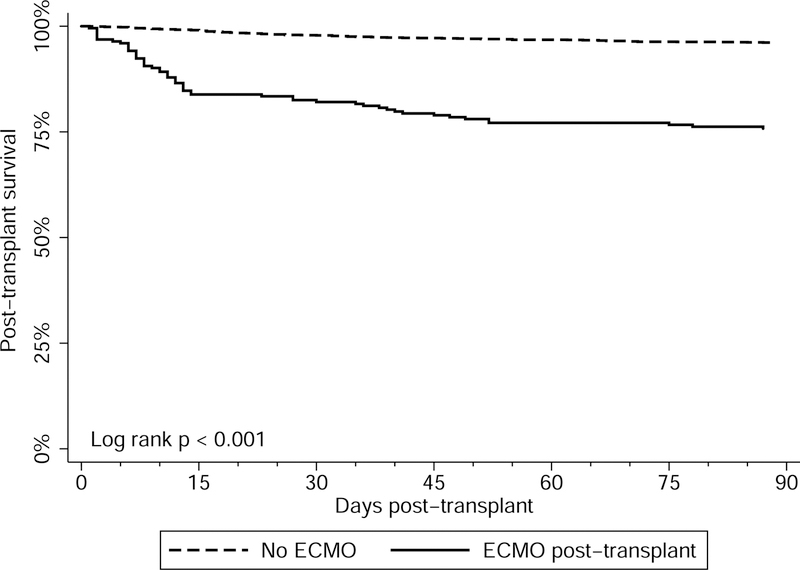
Primary graft dysfunction following HTx is associated with significant morbidity and mortality. This study aimed to assess the incidence of, risk factors for, and outcomes of children requiring ECMO within 24 hours of HTx. This study utilized a linked PHIS/SRTR database of pediatric HTx recipients (2002-2016). Post-HTx ECMO was identified using inpatient billing data. Logistic regression assessed risk factors for post-HTx ECMO. Kaplan-Meier analyses assessed in-hospital mortality and post-discharge survival. A total of 2820 patients were included with 224 (7.9%) requiring ECMO. Independent risk factors for post-HTx ECMO include age <1 year (aOR: 2.2, 95% CI: 1.3-3.7, P = 0.006) or 1-5 years (aOR: 2.1, 95% CI: 1.3-3.4, P = 0.002), and ECMO support at HTx (aOR: 27.4, 95% CI: 15.2-49.6, P < 0.001). Survival to discharge decreased with increasing duration of post-HTx ECMO support; 89% for 1-3 days, 79.1% for 4-6 days, 63.2% for 7-9 days, and 18.8% for ≥10 days. There was no difference in long-term survival for patients requiring post-HTx ECMO who survived to hospital discharge (P = 0.434). There are identifiable risk factors associated with the need for ECMO in the post-HTx period. Length of time on ECMO post-HTx is strongly associated with the risk of in-hospital mortality. Patients who require ECMO early post-HTx and survive to discharge have comparable outcomes to patients who did not require ECMO.
Keywords: extracorporeal membrane oxygenation; graft failure; graft function; pediatric heart transplant.
© 2019 Wiley Periodicals, Inc.
Figures



References
-
- Rossano JW, Cherikh WS, Chambers DC, et al. The Registry of the International Society for Heart and Lung Transplantation: Twentieth Pediatric Heart Transplantation Report-2017; Focus Theme: Allograft ischemic time. J Heart Lung Transplant 2017;36(10):1060–1069. - PubMed
-
- Kaushal S, Matthews KL, Garcia X, et al. A multicenter study of primary graft failure after infant heart transplantation: impact of extracorporeal membrane oxygenation on outcomes. Pediatr Transplant 2014;18(1):72–78. - PubMed
-
- Mitchell MB, Campbell DN, Bielefeld MR, Doremus T. Utility of extracorporeal membrane oxygenation for early graft failure following heart transplantation in infancy. J Heart Lung Transplant 2000;19(9):834–839. - PubMed
-
- Perri G, Hasan A, Cassidy J, et al. Mechanical circulatory support after paediatric heart transplantation. Eur J Cardiothorac Surg 2012;42(4):696–701. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
