

Optimal management of gastroesophageal junction cancer
- PMID: 30973648
- PMCID: PMC10172875
- DOI: 10.1002/cncr.32066
Optimal management of gastroesophageal junction cancer
Abstract
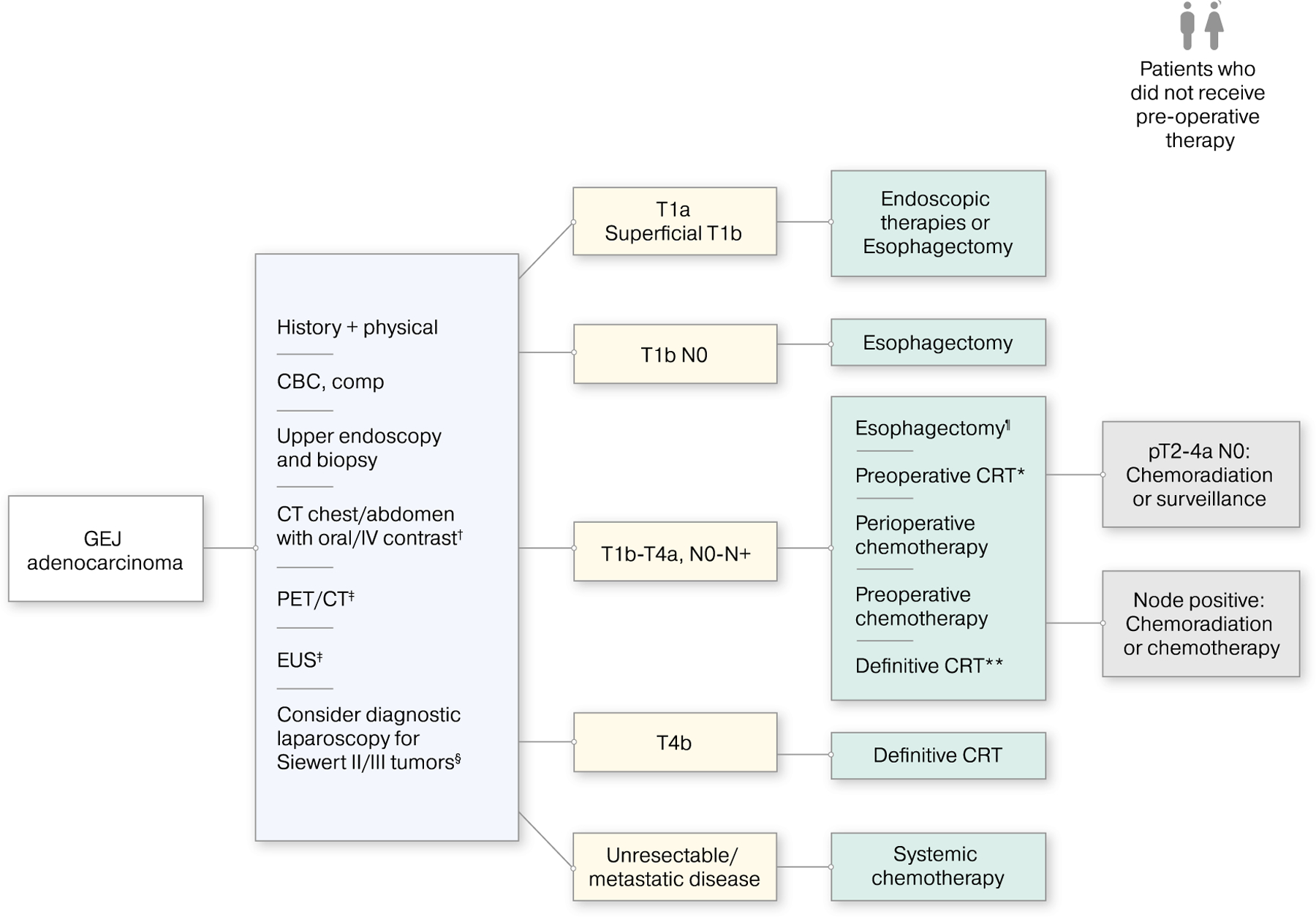
Although recent decades have witnessed incremental improvements in the treatment of gastroesophageal junction (GEJ) carcinoma, outcomes remain modest. For locally advanced esophageal cancer, the addition of chemotherapy and/or radiation to surgery is considered the standard of care. Chemotherapy remains the primary treatment for metastatic disease and improves survival over best supportive care. However, the prognosis for patients with GEJ cancers, which are treated along the same paradigms as esophageal and gastric carcinomas, remain poor because of the emergence of chemoresistance and limited targeted therapeutic approaches, which include agents that target the HER2 and vascular endothelial growth factor pathways. Evaluation of immune checkpoint inhibitors in the chemorefractory setting have confirmed the activity of immunotherapy in esophagogastric cancer. Ongoing immunotherapeutic strategies are being evaluated in both the locally advanced and metastatic settings. This review focuses on the treatment of locally advanced and metastatic GEJ carcinomas, which encompass all tumors that have an epicenter within 5 cm proximal or distal to the anatomical Z-line (Siewert classification). Because the vast majority of GEJ tumors are adenocarcinoma, the management of adenocarcinoma is the focus of this review. Evolving approaches and areas of clinical equipoise are discussed.
Keywords: (18F)2-fluoro-deoxy-D-glucose positron emission tomography (FDG-PET); adenocarcinoma; chemoradiation; chemotherapy; gastroesophageal junction cancer; immunotherapy; targeted therapy.
© 2019 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
David. H. Ilson is a consultant/advisory board member for Taiho, Pieris, Roche, Astra-Zeneca, Bayer, Bristol-Myers Squibb, Merck, and Astellas. The remaining other authors report no conflicts of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Arnold M, Laversanne M, Brown LM, Devesa SS, Bray F. Predicting the future burden of esophageal cancer by histological subtype: international trends in incidence up to 2030. Am J Gastroenterol 2017;112:1247–1255. - PubMed
-
- Mariette C, Dahan L, Mornex F, et al. Surgery alone versus chemoradiotherapy followed by surgery for stage I and II esophageal cancer: final analysis of randomized controlled phase III trial FFCD 9901. J Clin Oncol 2014;32:2416–2422. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 2006;355:11–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
