

Randomized Placebo Controlled Trial of Low-Dose Tamoxifen to Prevent Local and Contralateral Recurrence in Breast Intraepithelial Neoplasia
- PMID: 30973790
- PMCID: PMC6601429
- DOI: 10.1200/JCO.18.01779
Randomized Placebo Controlled Trial of Low-Dose Tamoxifen to Prevent Local and Contralateral Recurrence in Breast Intraepithelial Neoplasia
Abstract
Purpose: Tamoxifen administered for 5 years at 20 mg/d is effective in breast cancer treatment and prevention, but toxicity has limited its broad use. Biomarker trials showed that 5 mg/d is not inferior to 20 mg/d in decreasing breast cancer proliferation. We hypothesized that a lower dose given for a shorter period could be as effective in preventing recurrence from breast intraepithelial neoplasia but have a lower toxicity than the standard dose.
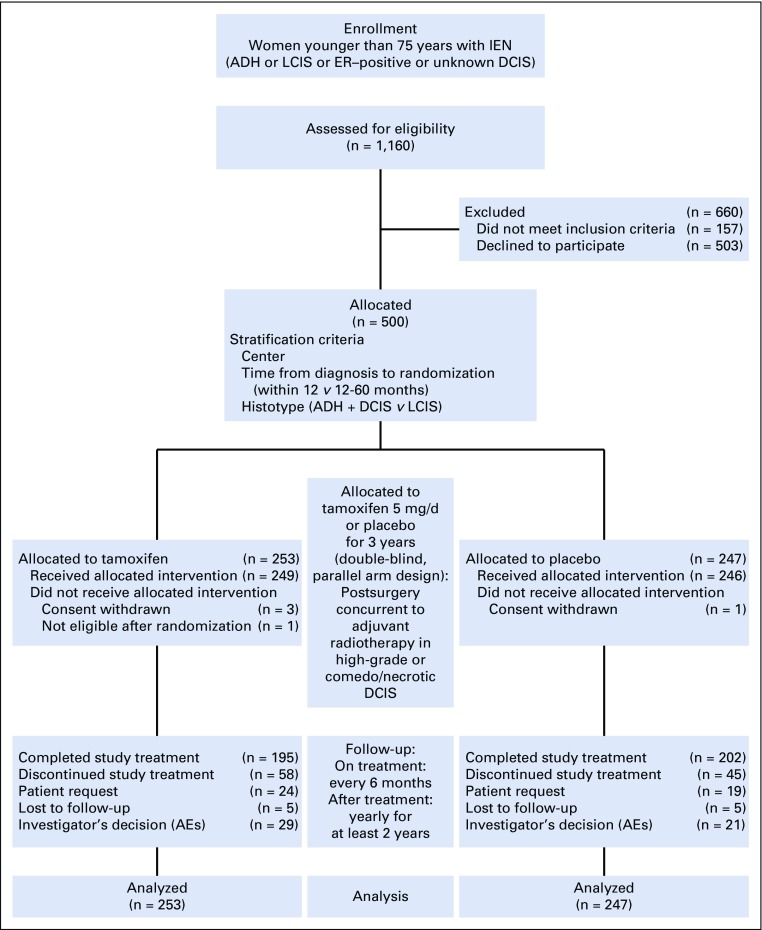
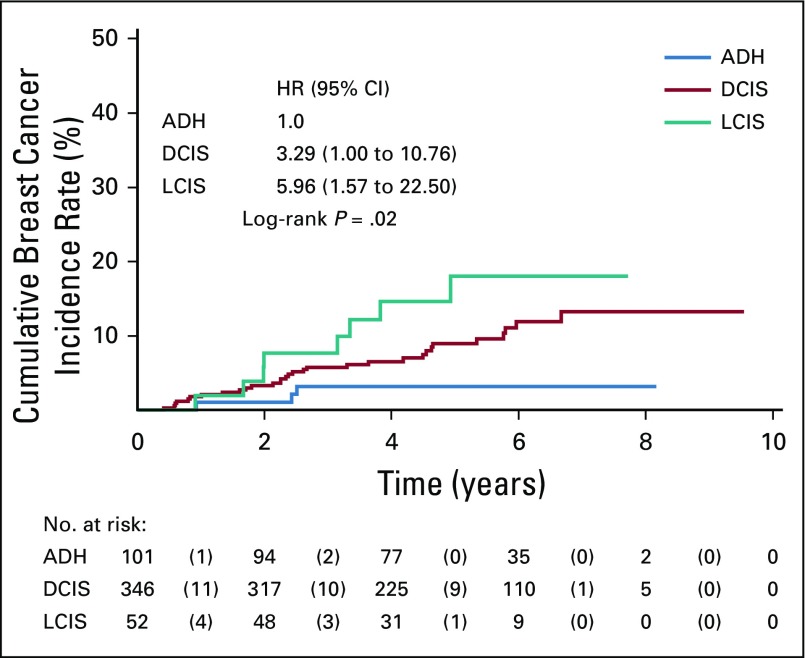
Patients and methods: We conducted a multicenter randomized trial of tamoxifen, 5 mg/d or placebo administered for 3 years after surgery in women with hormone-sensitive or unknown breast intraepithelial neoplasia, including atypical ductal hyperplasia and lobular or ductal carcinoma in situ. The primary end point was the incidence of invasive breast cancer or ductal carcinoma in situ.
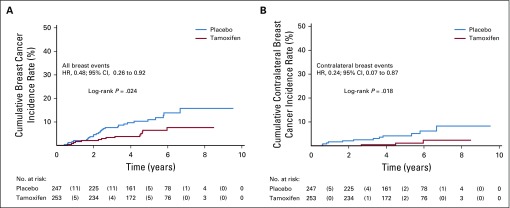
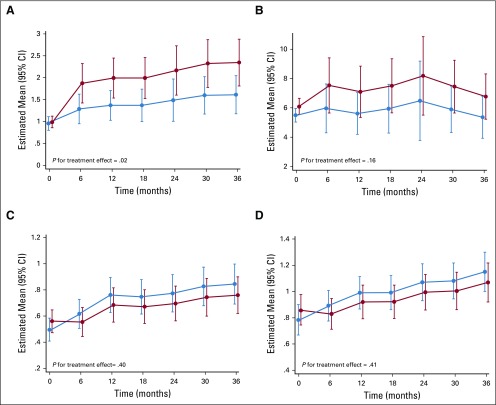
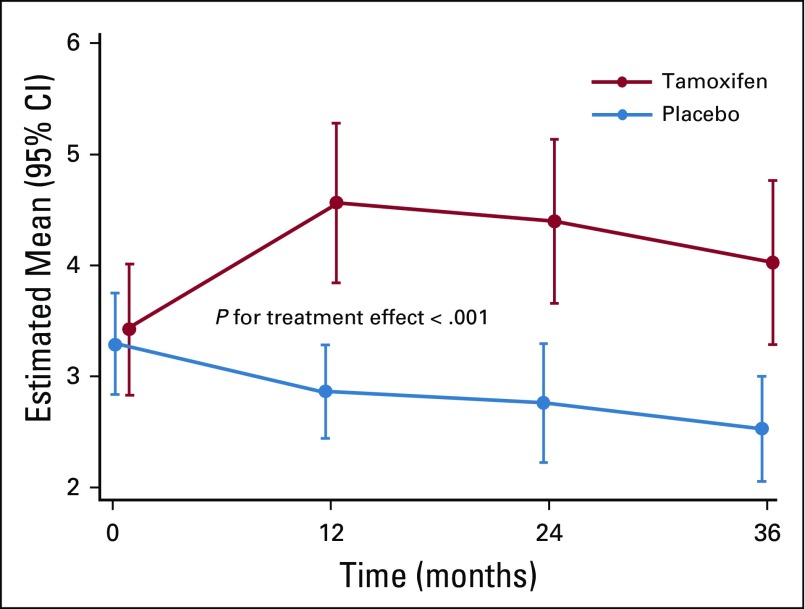
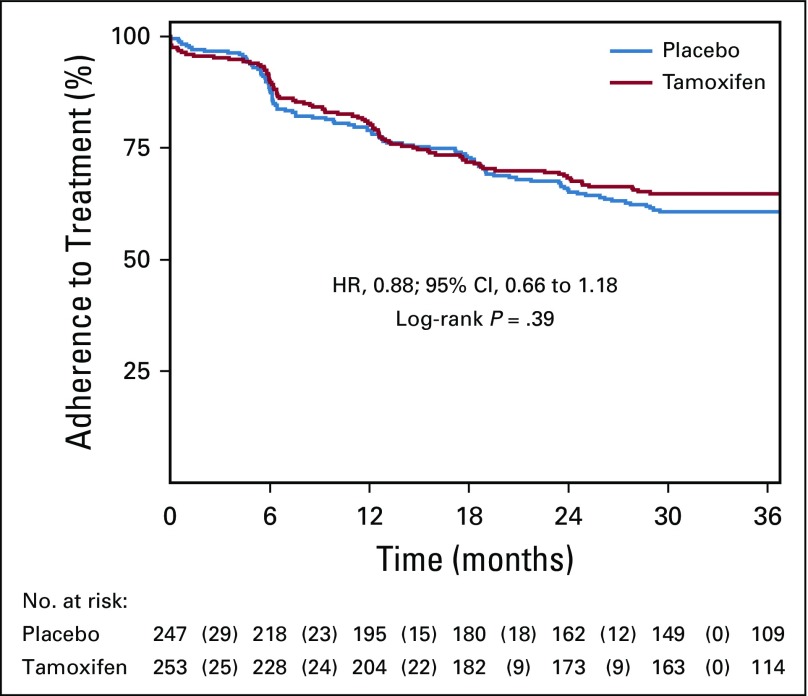
Results: Five hundred women 75 years of age or younger were included. After a median follow-up of 5.1 years (interquartile range, 3.9-6.3 years), there were 14 neoplastic events with tamoxifen and 28 with placebo (11.6 v 23.9 per 1,000 person-years; hazard ratio, 0.48; 95% CI, 0.26 to 0.92; P = .02), which resulted in a 5-year number needed to treat of 22 (95% CI, 20 to 27). Tamoxifen decreased contralateral breast events by 75% (three v 12 events; hazard ratio, 0.25; 95% CI, 0.07 to 0.88; P = .02). Patient-reported outcomes were not different between arms except for a slight increase in frequency of daily hot flashes with tamoxifen (P = .02). There were 12 serious adverse events with tamoxifen and 16 with placebo, including one deep vein thrombosis and one stage I endometrial cancer with tamoxifen and one pulmonary embolism with placebo.
Conclusion: Tamoxifen at 5 mg/d for 3 years can halve the recurrence of breast intraepithelial neoplasia with a limited toxicity, which provides a new treatment option in these disorders.
Trial registration: ClinicalTrials.gov NCT01357772.
Figures
Comment in
-
Will a Low-Dose Option Improve Uptake of Tamoxifen for Breast Cancer Risk Reduction?J Clin Oncol. 2019 Jul 1;37(19):1595-1597. doi: 10.1200/JCO.19.00656. Epub 2019 May 13. J Clin Oncol. 2019. PMID: 31082270 No abstract available.
References
-
- Lazzeroni M, Dunn BK, Pruneri G, et al. Adjuvant therapy in patients with ductal carcinoma in situ of the breast: The Pandora’s box. Cancer Treat Rev. 2017;55:1–9. - PubMed
-
- Merrill AL, Esserman L, Morrow M. Ductal carcinoma in situ. N Engl J Med. 2016;374:390–392. - PubMed
-
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: Report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371–1388. - PubMed
-
- Noonan S, Pasa A, Fontana V, et al. A survey among breast cancer specialists on the low uptake of therapeutic prevention with tamoxifen or raloxifene. Cancer Prev Res (Phila) 2018;11:38–43. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
