

Acute and 1-Year Hospitalization Costs for Acute Myocardial Infarction Treated With Percutaneous Coronary Intervention: Results From the TRANSLATE-ACS Registry
- PMID: 30975005
- PMCID: PMC6507213
- DOI: 10.1161/JAHA.118.011322
Acute and 1-Year Hospitalization Costs for Acute Myocardial Infarction Treated With Percutaneous Coronary Intervention: Results From the TRANSLATE-ACS Registry
Abstract
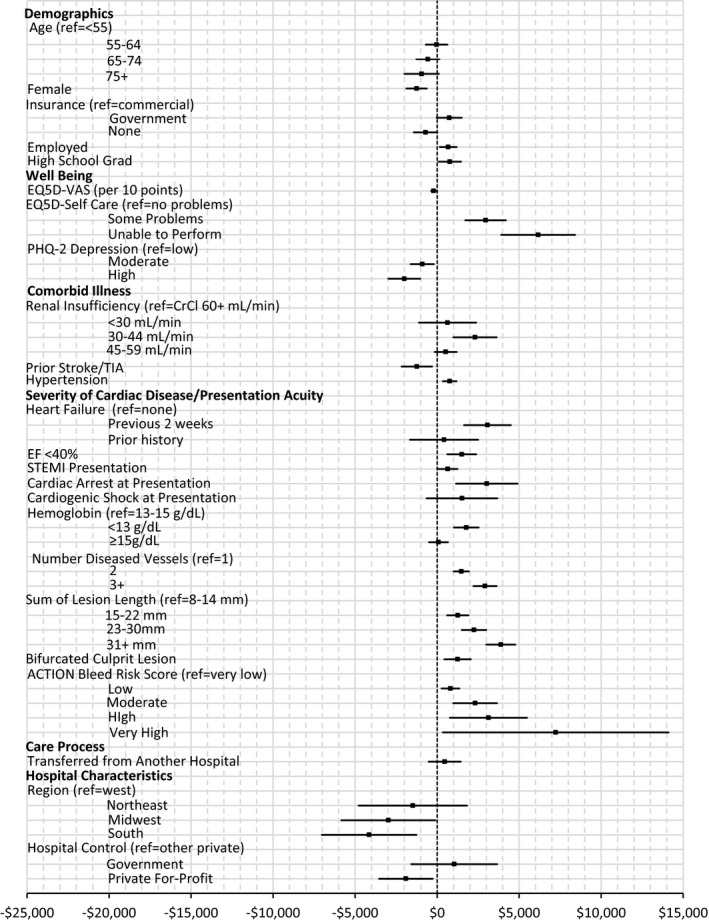
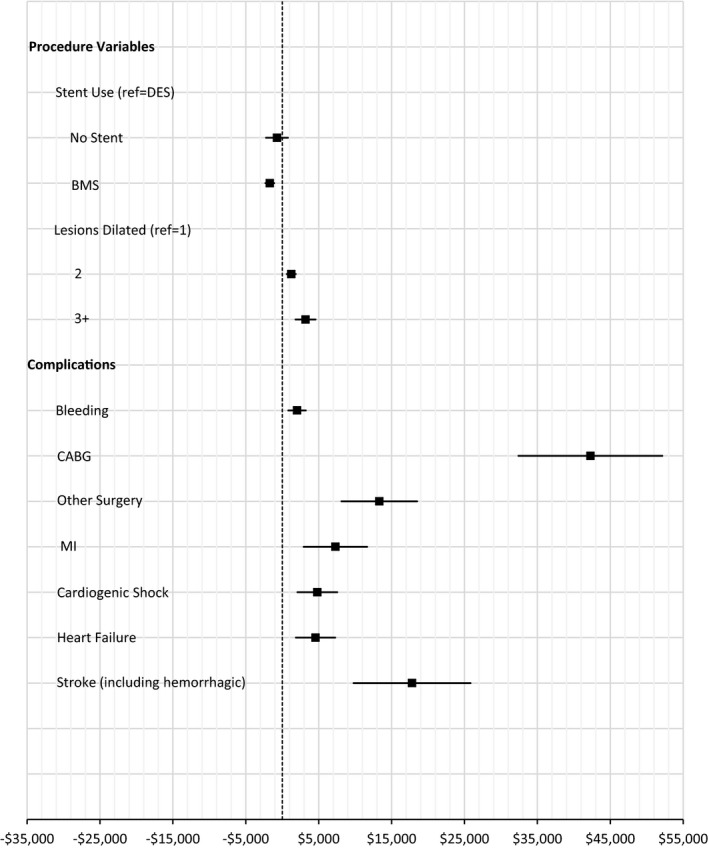
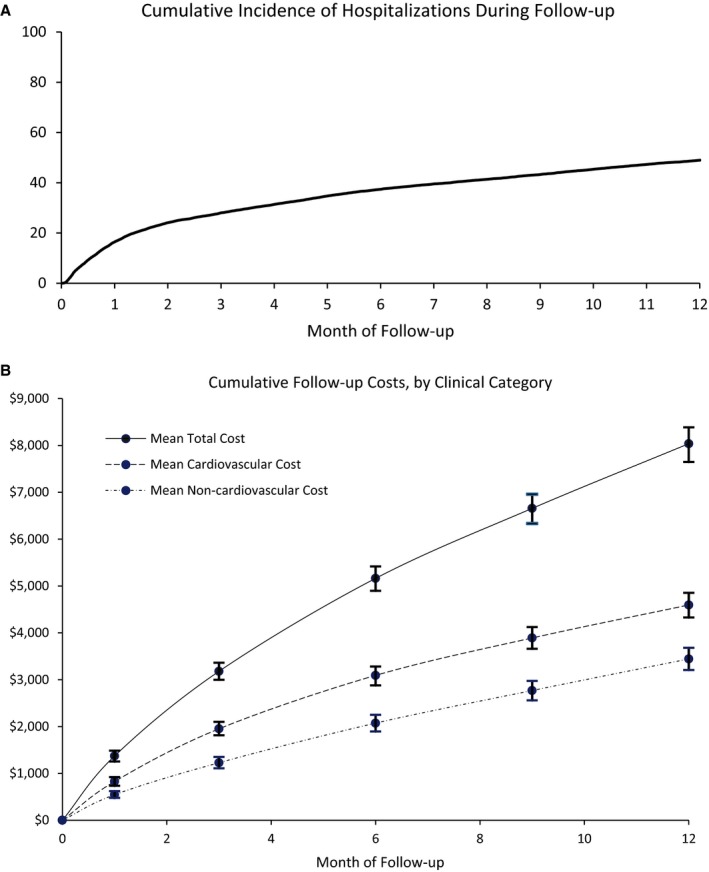
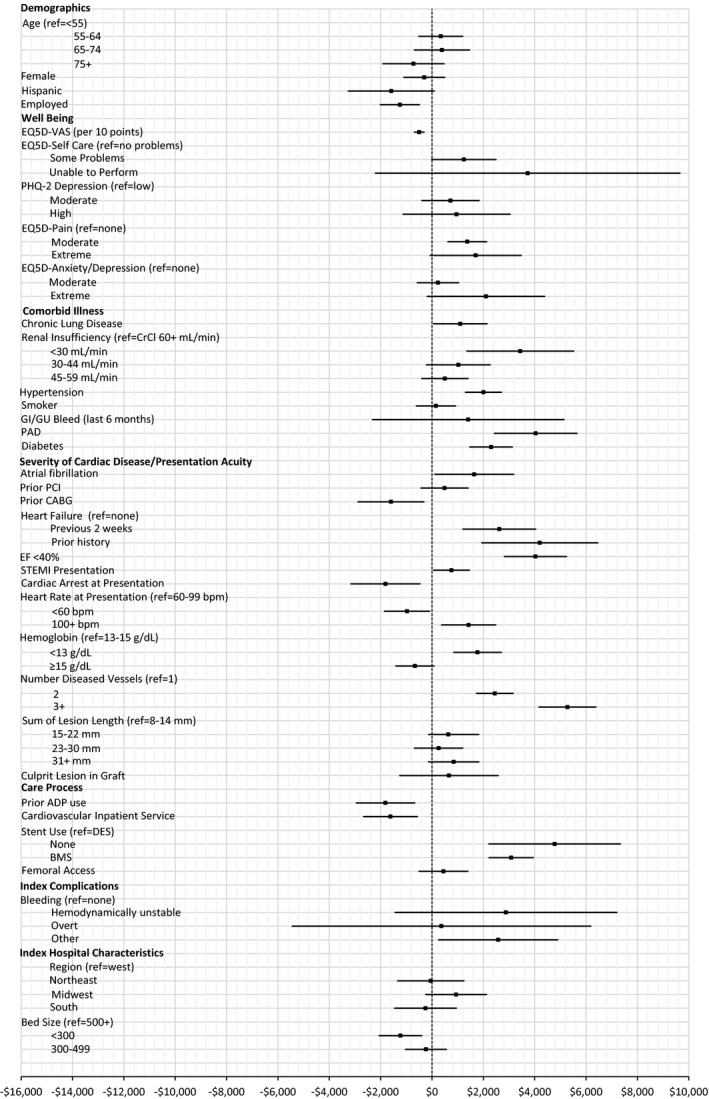
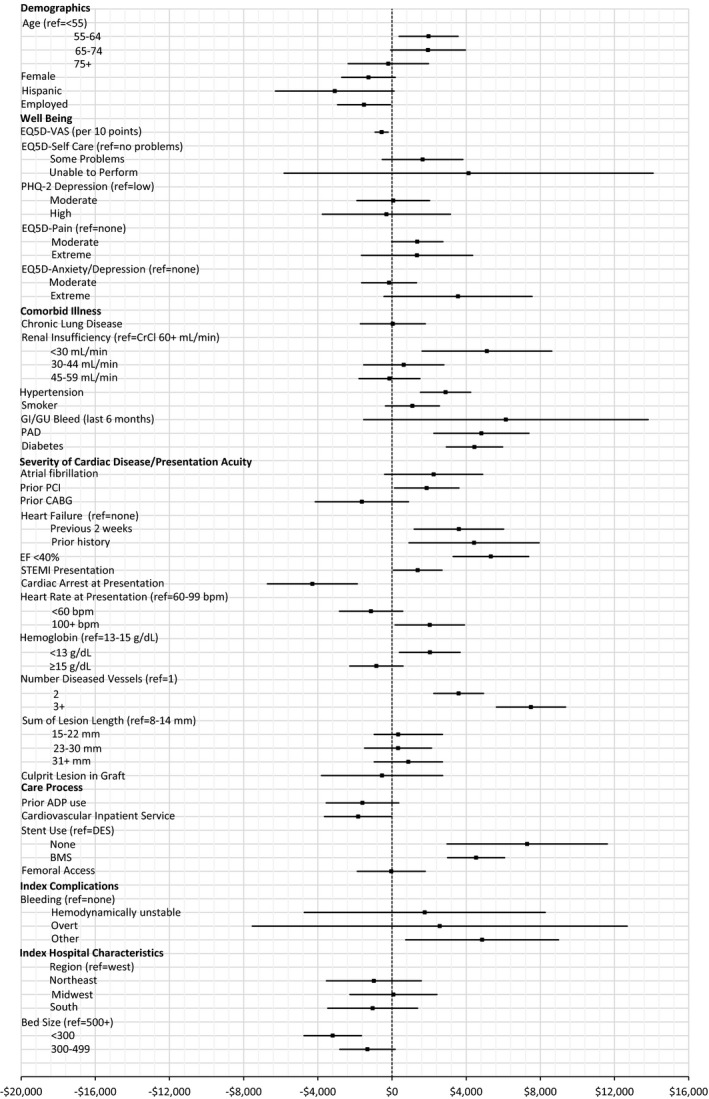
Background Hospitalization for acute myocardial infarction (MI) in the United States is both common and expensive, but those features alone provide little insight into cost-saving opportunities. Methods and Results To understand the cost drivers during hospitalization for acute MI and in the following year, we prospectively studied 11 969 patients with acute MI undergoing percutaneous coronary intervention at 233 US hospitals (2010-2013) from the TRANSLATE-ACS (Treatment With ADP Receptor Inhibitors: Longitudinal Assessment of Treatment Patterns and Events After Acute Coronary Syndrome) registry. Baseline costs were collected in a random subset (n=4619 patients, 54% ST-segment-elevation MI [STEMI]), while follow-up costs out to 1 year were collected for all patients. The mean index length of stay was 3.1 days (for both STEMI and non-STEMI) and mean intensive care unit length of stay was 1.2 days (1.4 days for STEMI and 1.0 days for non-STEMI). Index hospital costs averaged $18 931 ($19 327 for STEMI, $18 465 for non-STEMI), with 45% catheterization laboratory-related and 20% attributable to postprocedure hospital stay. Patient factors, including severity of illness and extent of coronary disease, and hospital characteristics, including for profit status and geographic region, identified significant variations in cost. Intensive care was used for 53% of non-STEMI and increased costs by $3282. Postdischarge 1-year costs averaged $8037, and 48% of patients were rehospitalized (half within 2 months and 57% with a cardiovascular diagnosis). Conclusions While much of the cost of patients with acute MI treated with percutaneous coronary intervention is probably not modifiable by the care team, cost reductions are still possible through quality-preserving practice efficiencies, such as need-based use rather than routine use of intensive care unit for patients with stable non-STEMI. Clinical Trial Registration URL: https://www.clinicaltrials.gov . Unique identifier: NCT00097591.
Keywords: acute myocardial infarction; cost; percutaneous coronary intervention.
Figures

Comment in
-
Reduce Acute Care Costs, and All Other Healthcare Costs Too.J Am Heart Assoc. 2019 Apr 16;8(8):e012604. doi: 10.1161/JAHA.119.012604. J Am Heart Assoc. 2019. PMID: 30975013 Free PMC article.
References
-
- Torio C, Moore B. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013. HCUP Statistical Brief #204. May 2016. Rockville, MD: Agency for Healthcare Research and Quality; 2013. Available at: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive-Hos.... Accessed January 29, 2019. - PubMed
-
- Sugiyama T, Hasegawa K, Kobayashi Y, Takahashi O, Fukui T, Tsugawa Y. Differential time trends of outcomes and costs of care for acute myocardial infarction hospitalizations by ST elevation and type of intervention in the United States, 2001–2011. J Am Heart Assoc. 2015;4:e001445 DOI: 10.1161/JAHA.114.001445 - DOI - PMC - PubMed
-
- Kaplan RS, Haas DA. How not to cut health care costs. Harv Bus Rev. 2014;92:142. - PubMed
-
- Kaplan RS, Porter ME. How to solve the cost crisis in health care. Harv Bus Rev. 2011;89:46–52, 54, 56‐61 passim. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
