

Protective ventilation with high versus low positive end-expiratory pressure during one-lung ventilation for thoracic surgery (PROTHOR): study protocol for a randomized controlled trial
- PMID: 30975217
- PMCID: PMC6460685
- DOI: 10.1186/s13063-019-3208-8
Protective ventilation with high versus low positive end-expiratory pressure during one-lung ventilation for thoracic surgery (PROTHOR): study protocol for a randomized controlled trial
Erratum in
-
Correction to: Protective ventilation with high versus low positive end-expiratory pressure during one-lung ventilation for thoracic surgery (PROTHOR): study protocol for a randomized controlled trial.Trials. 2019 May 8;20(1):259. doi: 10.1186/s13063-019-3371-y. Trials. 2019. PMID: 31068212 Free PMC article.
Abstract
Background: Postoperative pulmonary complications (PPC) may result in longer duration of in-hospital stay and even mortality. Both thoracic surgery and intraoperative mechanical ventilation settings add considerably to the risk of PPC. It is unclear if one-lung ventilation (OLV) for thoracic surgery with a strategy of intraoperative high positive end-expiratory pressure (PEEP) and recruitment maneuvers (RM) reduces PPC, compared to low PEEP without RM.
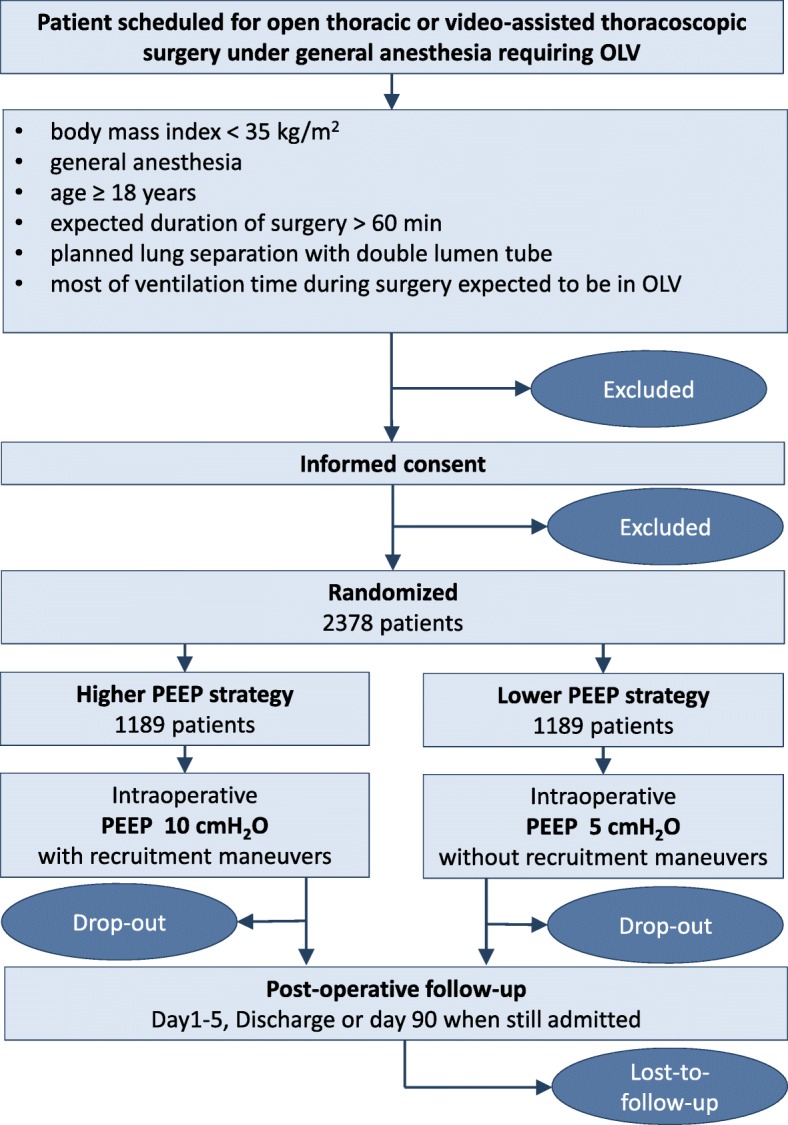
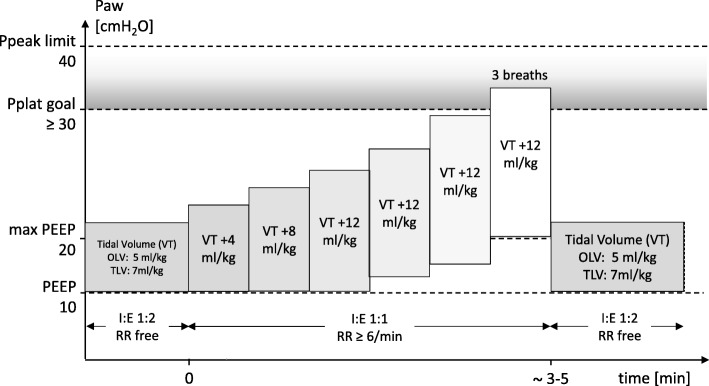
Methods: PROTHOR is an international, multicenter, randomized, controlled, assessor-blinded, two-arm trial initiated by investigators of the PROtective VEntilation NETwork. In total, 2378 patients will be randomly assigned to one of two different intraoperative mechanical ventilation strategies. Investigators screen patients aged 18 years or older, scheduled for open thoracic or video-assisted thoracoscopic surgery under general anesthesia requiring OLV, with a maximal body mass index of 35 kg/m2, and a planned duration of surgery of more than 60 min. Further, the expected duration of OLV shall be longer than two-lung ventilation, and lung separation is planned with a double lumen tube. Patients will be randomly assigned to PEEP of 10 cmH2O with lung RM, or PEEP of 5 cmH2O without RM. During two-lung ventilation tidal volume is set at 7 mL/kg predicted body weight and, during OLV, it will be decreased to 5 mL/kg. The occurrence of PPC will be recorded as a collapsed composite of single adverse pulmonary events and represents the primary endpoint.
Discussion: PROTHOR is the first randomized controlled trial in patients undergoing thoracic surgery with OLV that is adequately powered to compare the effects of intraoperative high PEEP with RM versus low PEEP without RM on PPC. The results of the PROTHOR trial will support anesthesiologists in their decision to set intraoperative PEEP during protective ventilation for OLV in thoracic surgery.
Trial registration: The trial was registered in clinicaltrials.gov ( NCT02963025 ) on 15 November 2016.
Keywords: Mechanical ventilation; one-lung ventilation; positive end-expiratory pressure; postoperative pulmonary complication; recruitment maneuver; thoracic surgery.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The Istanbul University, Medical Faculty, Ethical Committee of clinical research approved the study on 08.04.2016 (File number 2016/483, study protocol version 1.9). Additionally, the institutional review board at the University Hospital Dresden, Technische Universität Dresden, Dresden, Germany, approved the study on 23.09.2016 (reference no. EK 392092016, study protocol version 1.9). The respective review boards of participating sites also approved the study. PROTHOR is designed in accordance to the principles of the Declaration of Helsinki. Written informed consent was obtained from every enrolled patient upon request by the local institutional review board.
Consent for publication
Not applicable.
Competing interests
MRET received free airway device samples from Ambu in April 2014 and from Airtraq in March 2015 for use in another three published studies. He has no direct financial or other interests in Ambu or Airtraq (in the context of this and his studies).
All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Canet J, Sabate S, Mazo V, Gallart L, de Abreu MG, Belda J, et al. Development and validation of a score to predict postoperative respiratory failure in a multicentre European cohort: A prospective, observational study. Eur J Anaesthesiol. 2015;32(7):458–470. doi: 10.1097/EJA.0000000000000223. - DOI - PubMed
-
- Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med. 2014;2(12):1007–1015. doi: 10.1016/S2213-2600(14)70228-0. - DOI - PubMed
-
- Guldner A, Kiss T, Serpa Neto A, Hemmes SN, Canet J, Spieth PM, et al. Intraoperative protective mechanical ventilation for prevention of postoperative pulmonary complications: a comprehensive review of the role of tidal volume, positive end-expiratory pressure, and lung recruitment maneuvers. Anesthesiology. 2015;123(3):692–713. doi: 10.1097/ALN.0000000000000754. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
