

Vascular Access for Hemodialysis Patients: New Data Should Guide Decision Making
- PMID: 30975657
- PMCID: PMC6556719
- DOI: 10.2215/CJN.00490119
Vascular Access for Hemodialysis Patients: New Data Should Guide Decision Making
Abstract
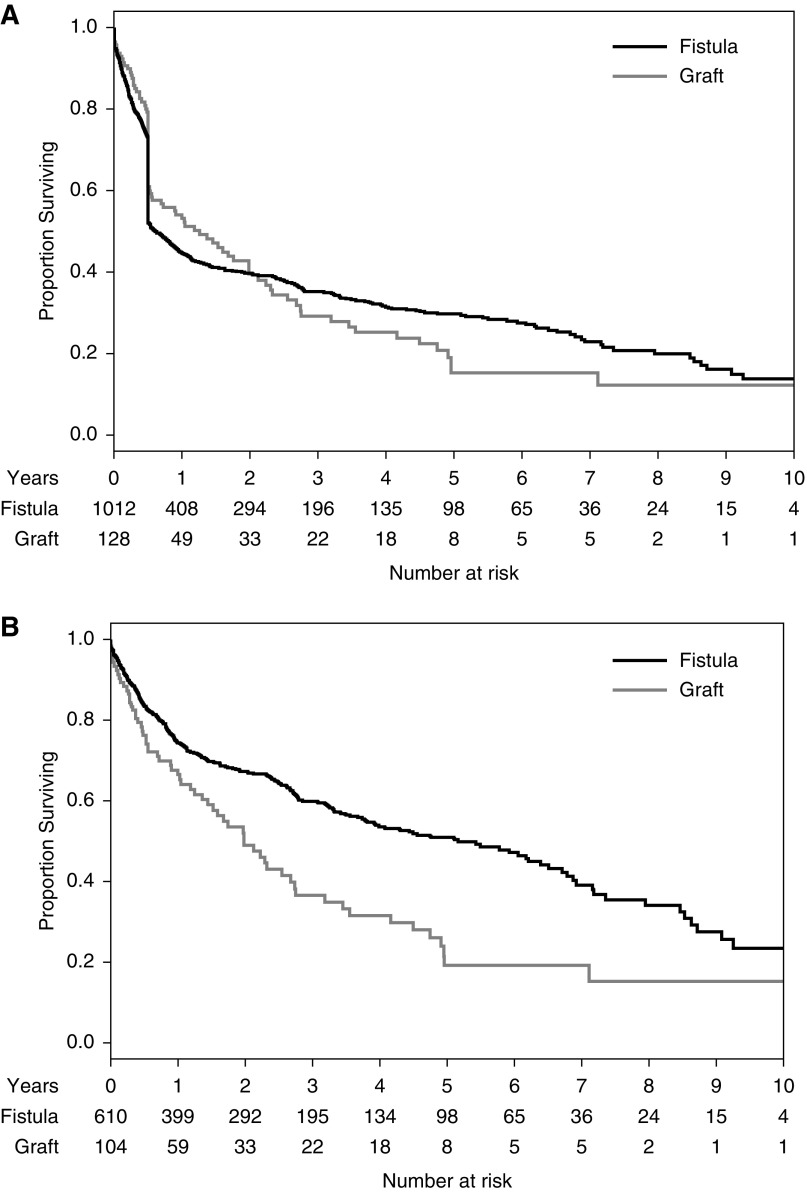
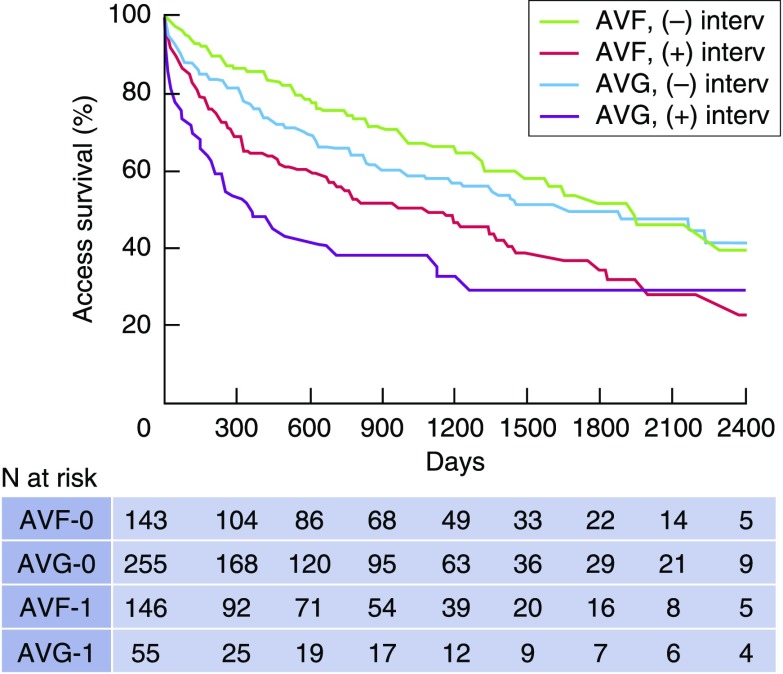
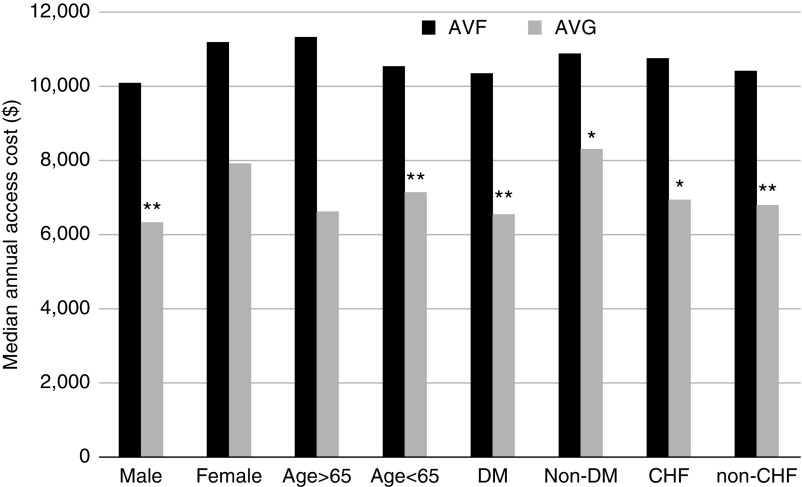
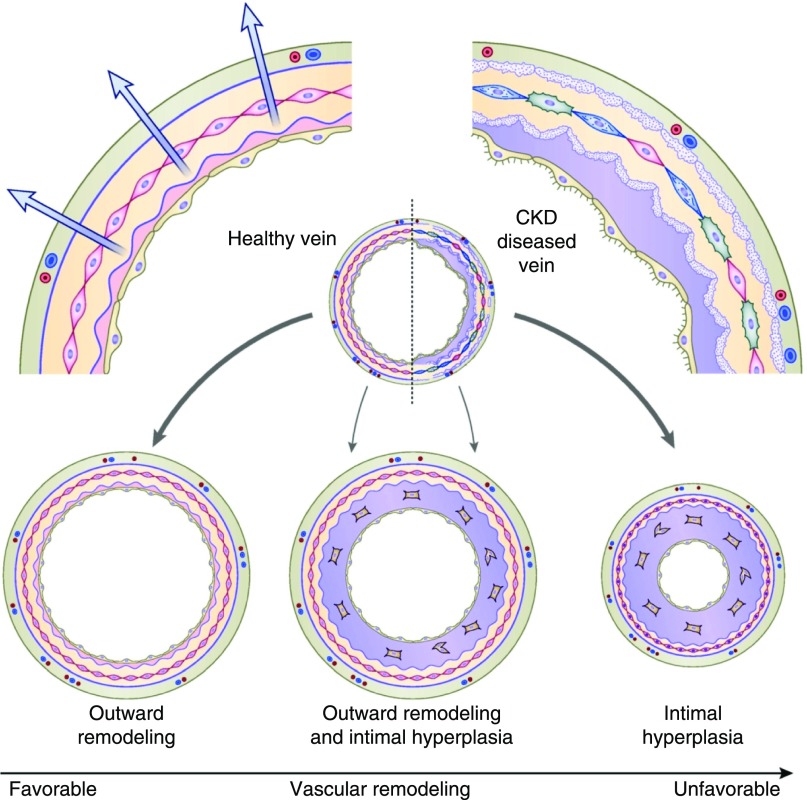
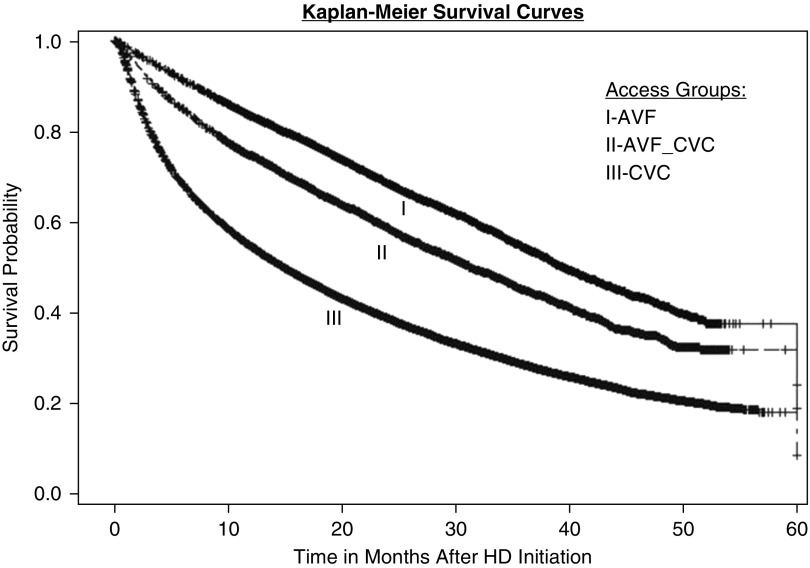
This commentary critically examines key assumptions and recommendations in the 2006 Kidney Disease Outcomes Quality Initiative vascular access guidelines, and argues that several are not relevant to the contemporary United States hemodialysis population. First, the guidelines prefer arteriovenous fistulas (AVFs) over arteriovenous grafts (AVGs), on the basis of their superior secondary survival and lower frequency of interventions and infections. However, intent-to-treat analyses that incorporate the higher primary failure of AVFs, demonstrate equivalent secondary survival of both access types. Moreover, the lower rate of AVF versus AVG infections is counterbalanced by the higher rate of catheter-related bloodstream infections before AVF maturation. In addition, AVFs with assisted maturation (interventions before successful AVF use), which account for about 50% of new AVFs, are associated with inferior secondary patency compared with AVGs without intervention before successful use. Second, the guidelines posit lower access management costs for AVFs than AVGs. However, in patients who undergo AVF or AVG placement after starting dialysis with a central venous catheter (CVC), the overall cost of access management is actually higher in patients receiving an AVF. Third, the guidelines prefer forearm over upper arm AVFs. However, published data demonstrate superior maturation of upper arm versus forearm AVFs, likely explaining the progressive increase in upper arm AVFs in the United States. Fourth, AVFs are thought to fail primarily because of aggressive juxta-anastomotic stenosis. However, recent evidence suggests that many AVFs mature despite neointimal hyperplasia, and that suboptimal arterial vasodilation may be an equally important contributor to AVF nonmaturation. Finally, CVC use is believed to result in excess mortality in patients on hemodialysis. However, recent data suggest that CVC use is simply a surrogate marker of sicker patients who are more likely to die, rather than being a mediator of mortality.
Keywords: Arteriovenous Shunt, Surgical; Bacteremia; Biomarkers; Catheter-Related Infections; Central Venous Catheters; Constriction, Pathologic; Decision Making; Forearm; Hyperplasia; Kidney Diseases; Vasodilation; arteriovenous fistula; arteriovenous graft; dialysis; dialysis catheter.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Maya ID, Allon M: Core curriculum in nephrology: Vascular access. Am J Kidney Dis 51: 702–708, 2008 - PubMed
-
- Vascular Access 2006 Work Group: Clinical practice guidelines for vascular access. Am J Kidney Dis 48: S176–S322, 2006 - PubMed
-
- Kinnaert P, Vereerstraeten P, Toussaint C, Van Geertruyden J: Nine years’ experience with internal arteriovenous fistulas for haemodialysis: A study of some factors influencing the results. Br J Surg 64: 242–246, 1977 - PubMed
-
- Bonalumi U, Civalleri D, Rovida S, Adami GF, Gianetta E, Griffanti-Bartoli F: Nine years’ experience with end-to-end arteriovenous fistula at the ‘anatomical snuffbox’ for maintenance haemodialysis. Br J Surg 69: 486–488, 1982 - PubMed
-
- Reilly DT, Wood RFM, Bell PRF: Prospective study of dialysis fistulas: Problem patients and their treatment. Br J Surg 69: 549–553, 1982 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
