

Eculizumab prevents thrombotic microangiopathy in patients with atypical haemolytic uraemic syndrome in a long-term observational study
- PMID: 30976396
- PMCID: PMC6452204
- DOI: 10.1093/ckj/sfy035
Eculizumab prevents thrombotic microangiopathy in patients with atypical haemolytic uraemic syndrome in a long-term observational study
Abstract
Background: Eculizumab, a terminal complement inhibitor, is approved for atypical haemolytic uraemic syndrome (aHUS) to inhibit complement-mediated thrombotic microangiopathy (TMA).
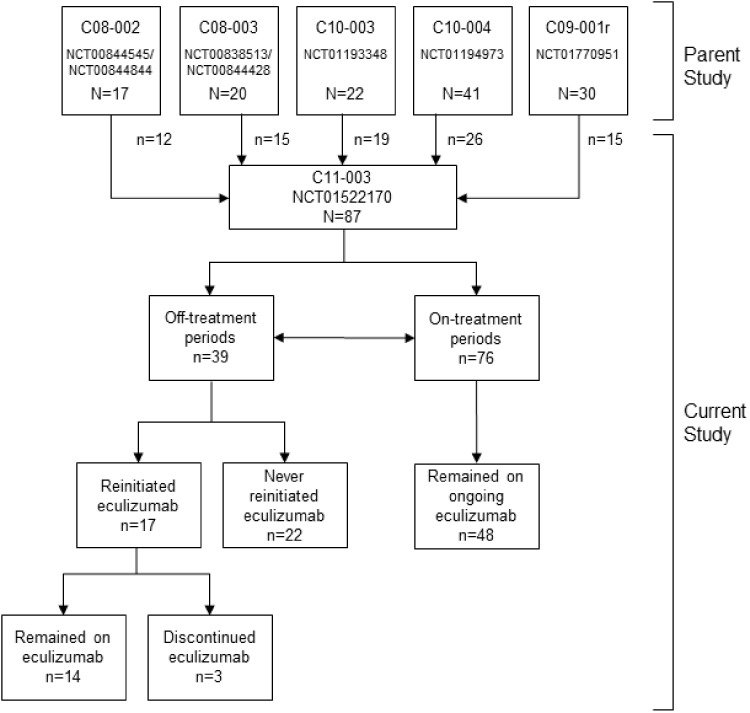
Methods: In five parent studies, eculizumab effectively prevented TMA and improved renal and haematologic outcomes in patients with aHUS; therefore, these patients could enrol in this long-term, prospective, observational and multicentre study. The primary endpoint was the TMA manifestation rate off and on eculizumab post-parent study. Post hoc analyses evaluated rates during labelled versus non-labelled dosing regimens, and in those with versus without identified complement abnormalities. Serious targeted treatment-emergent adverse events (TEAEs) were evaluated.
Results: Of 87 patients in the current study, 39 and 76 had off- and on-treatment periods, respectively; 17 (44%) with off periods reinitiated eculizumab. TMA manifestation rate per 100 patient-years was 19.9 off and 7.3 on treatment [hazard ratio (HR), 4.7; P = 0.0008]; rates were highest off treatment and lowest during labelled regimens. TMA manifestations with hospitalizations/serious AEs occurred more frequently off versus on treatment. TMA rates were higher among patients with identified complement abnormalities (HR, 4.5; P = 0.0082). Serious targeted TEAEs occurred at similar rates off and on treatment.
Conclusions: As expected, patients with aHUS have increased risk of TMA manifestations after discontinuation of eculizumab or in the setting of non-labelled eculizumab dosing. Collectively, results show that maintaining eculizumab treatment minimizes risk of TMA, particularly in patients with identified complement abnormalities. Future studies are needed to further characterize TMA and longer term outcomes on labelled or non-labelled eculizumab regimens and after discontinuation of treatment.
Keywords: atypical haemolytic uraemic syndrome; complement; discontinuation; eculizumab; observational study; thrombotic microangiopathy.
References
-
- Noris M, Remuzzi G.. Atypical hemolytic-uremic syndrome. N Engl J Med 2009; 361: 1676–1687 - PubMed
-
- Noris M, Mescia F, Remuzzi G.. STEC-HUS, atypical HUS and TTP are all diseases of complement activation. Nat Rev Nephrol 2012; 8: 622–633 - PubMed
-
- US Food and Drug Administration. Soliris (eculizumab) [Prescribing Information]. New Haven, CT: Alexion Pharmaceuticals, Inc, 2017
LinkOut - more resources
Full Text Sources
Research Materials
