

Review
doi: 10.21037/qims.2018.11.10.
Imaging of sacroiliitis: Current status, limitations and pitfalls
Affiliations
- PMID: 30976556
- PMCID: PMC6414763
- DOI: 10.21037/qims.2018.11.10
Item in Clipboard
Review
Imaging of sacroiliitis: Current status, limitations and pitfalls
Quant Imaging Med Surg.
2019 Feb.
Abstract
The clinical need to diagnose sacroiliitis at an earlier stage has led to the sacroiliac joints being more frequently imaged, particularly with magnetic resonance imaging (MRI). This review outlines the imaging approach to sacroiliitis, emphasizing the imaging protocols, diagnostic criteria, limitations and potential mimics of MRI examination. The value of imaging-guided intervention in sacroiliac joint disease is also briefly outlined.
Keywords: Sacroiliitis; imaging; magnetic resonance imaging (MRI); sacroiliac joints; spondyloarthritis (SpA).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
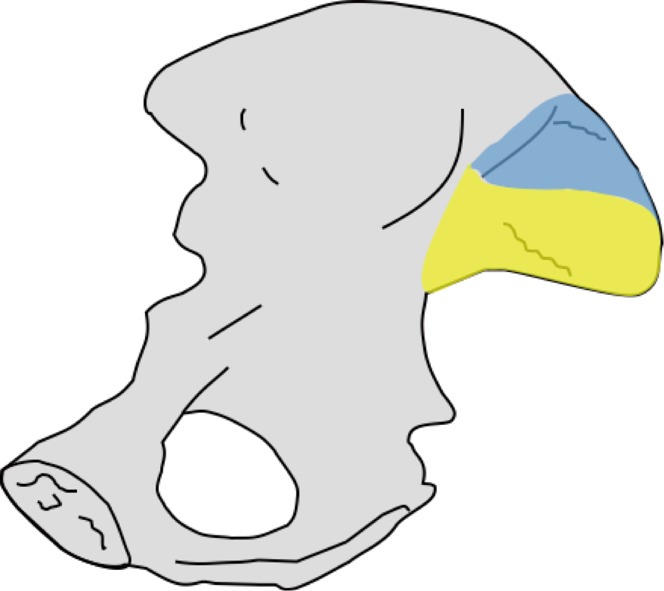
Looking at the iliac side of the SI joint, the synovial part (yellow) is located anteroinferiorly while the ligamentous part (blue) is located posterosuperiorly.
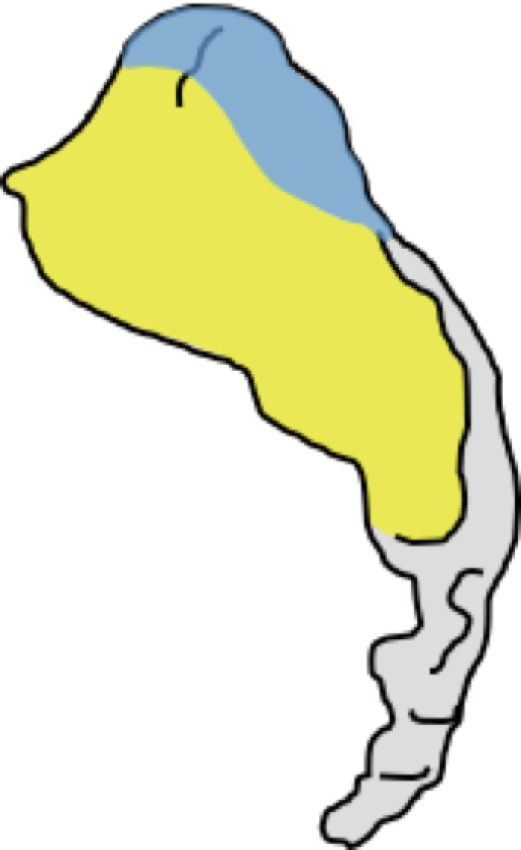
Looking at the sacral side of the SI joint, the synovial part (yellow) is located anteroinferiorly and the ligamentous part (blue) is located posterosuperiorly.
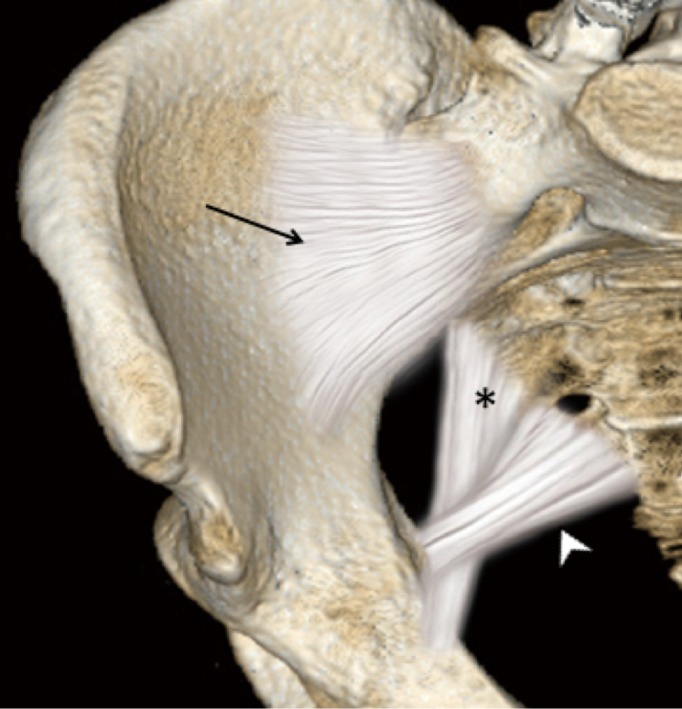
Nearly all of the anterior aspect of the sacroiliac joint is true synovial joint except for the uppermost anterior part which is syndesmotic. Additional extra-articular ligament support is provided by the anterior sacroiliac ligament (arrow), sacrospinous ligament (arrowhead), and sacrotuberous ligament (asterisk).
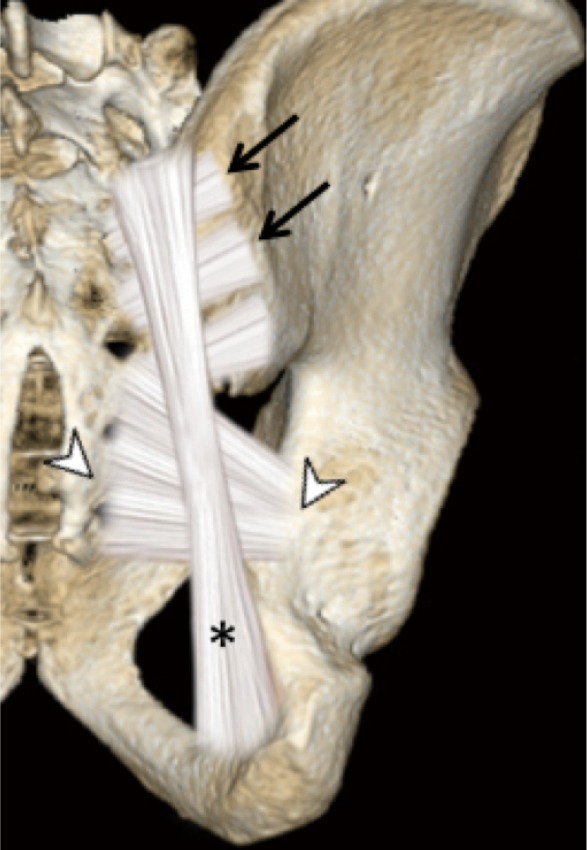
The posterior part of the upper and mid-sacroiliac joint is syndesmotic. The inferior part is synovial. Additional posterior support is provided by the extra-articular posterior sacroiliac ligament (arrows), sacrospinous ligament (arrowheads), and sacrotuberous ligament (asterisks).

Axial CT images showing the position of the synovial (yellow) and ligamentous (blue) components of the sacroiliac joint from (A) cranial, (B) mid- and (C) caudal aspects of the sacroiliac joints.
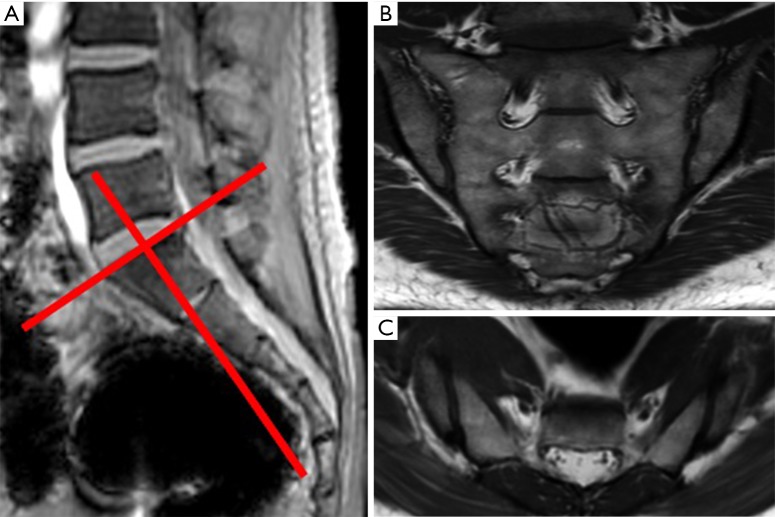
Sacroiliac joint MR imaging. (A) Sagittal scout view. On the sagittal scout view, an oblique coronal plane of the sacroiliac joints is planned along a plane perpendicular to the upper end plate of S1; (B) T1SE oblique coronal view mid-third sacroiliac joints; (C) T1SE oblique axial view of inferior one-third sacroiliac joints. The additional pick-up rate for sacroiliitis on oblique axial imaging is limited on top of the oblique coronal view.
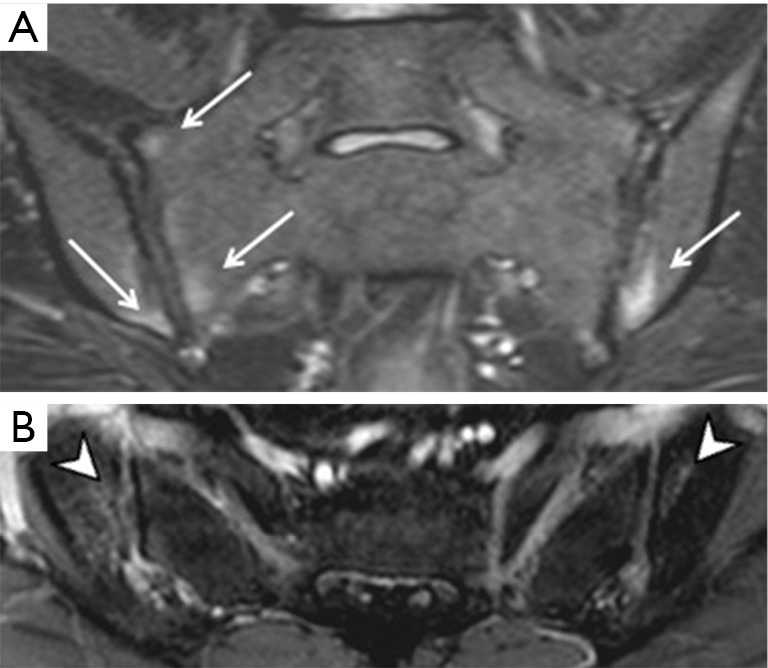
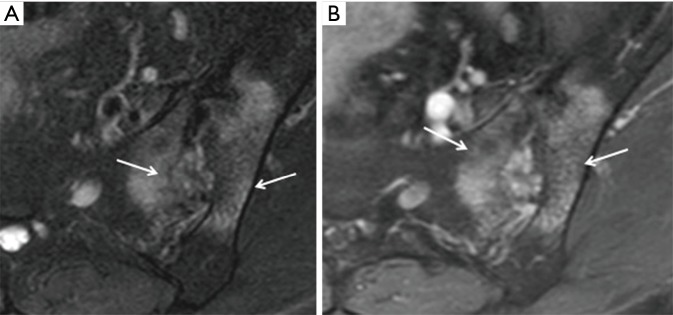
Sacroiliitis on MRI. (A) Bone marrow oedema (arrows) on T2W FS oblique coronal images and (B) corresponding enhancement (arrowheads) on T1W FS post-contrast axial images. This degree of bone marrow oedema is sufficient to diagnose sacroiliitis.
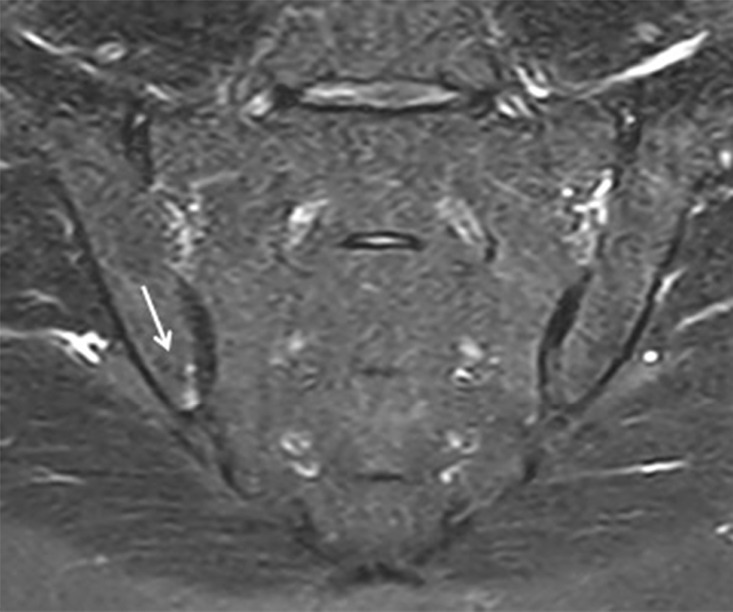
Small area of bone marrow oedema (arrow) and enhancement can be physiological or related to osteoarthritis or osteitis condensans ilii. For bone marrow oedema to be pathognomonic of sacroiliitis, it needs to be of >1 cm in width or depth and be apparent on more than 1 image or at 2 separate sites on the same image.
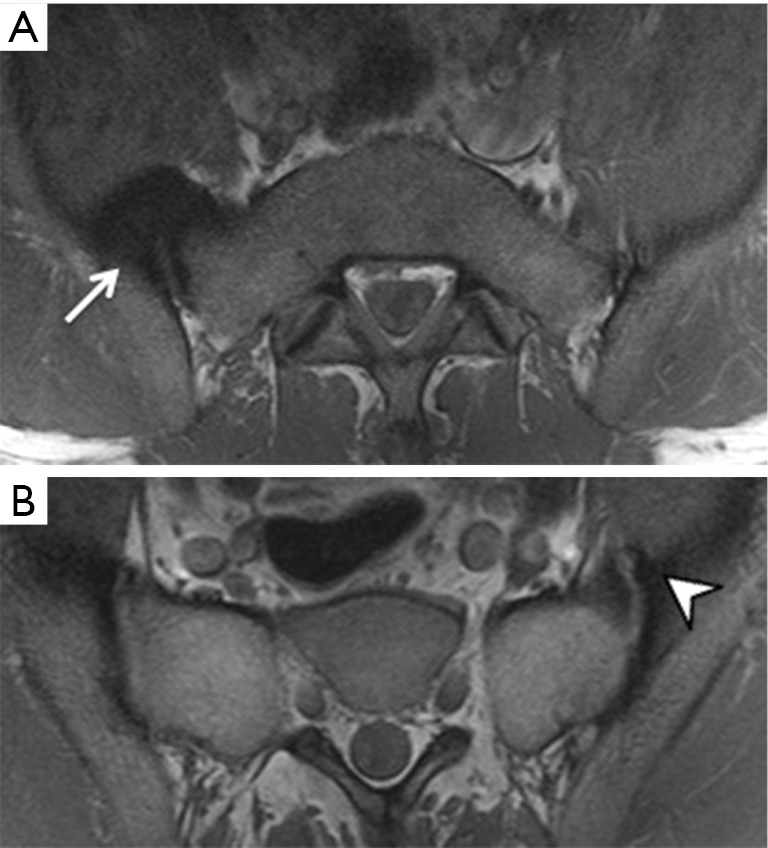
Capsulitis can be visible (A) anteriorly (arrow) or (B) posteriorly (arrowhead) and may extend to involve the adjacent bone. The presence of capsulitis alone is not diagnostic of spondyloarthropathy.
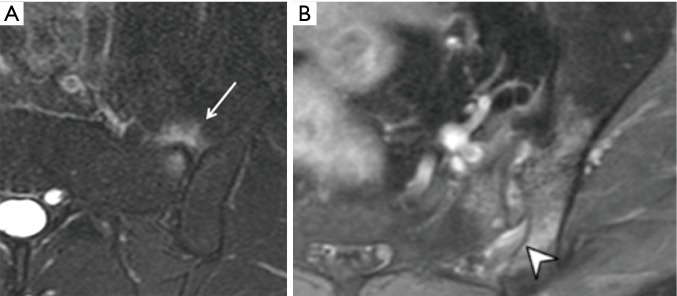
Enthesitis is a common finding in active sacroiliitis on (A) T2W STIR and (B) post-contrast T1W FS. Enthesitis is seen as ligamentous oedema, bony irregularity and bone marrow oedema (arrow) deep to areas of ligamentous insertion. Both the sacral and iliac sides can be involved. In this case, it occurs at the attachment of the interosseous ligament. Enthesitis can also be seen at muscular attachments and at the attachments of the extra-articular sacrospinous and sacrotuberous ligaments. The presence of enthesitis alone is not diagnostic of spondyloarthropathy.
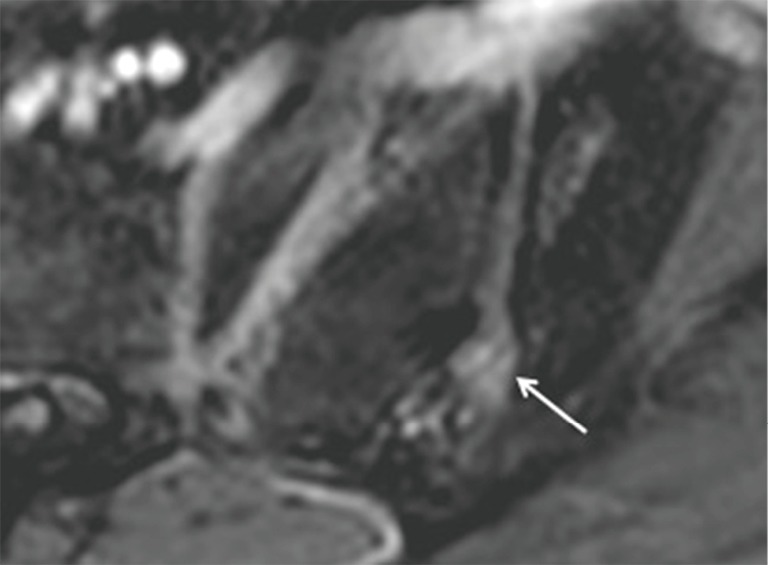
Synovitis (arrow) is best demonstrated on post-contrast images and should be differentiated from peri-articular vasculature by ensuring that the enhancement is seen on consecutive images.
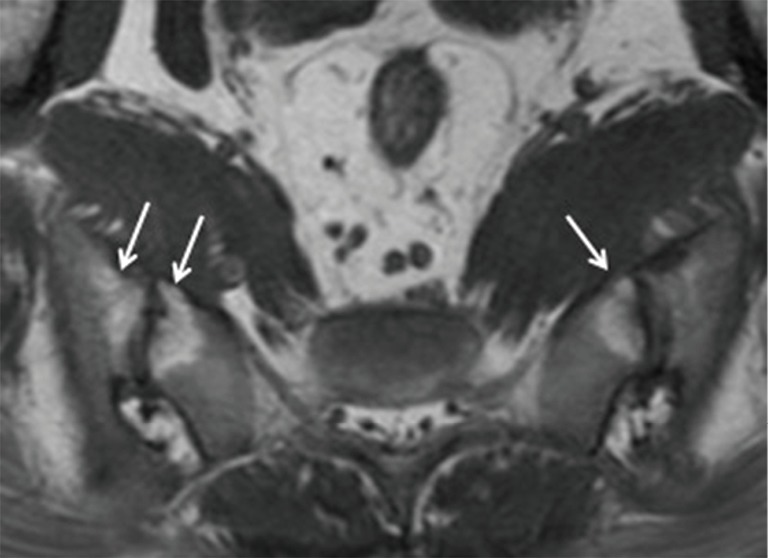
Peri-articular fatty deposition (arrows) can only be appreciated on MRI. This finding is suggestive of chronic sacroiliitis, but is non-specific, being also often seen in osteoarthritis and, less so, in osteitis condensans ilii.
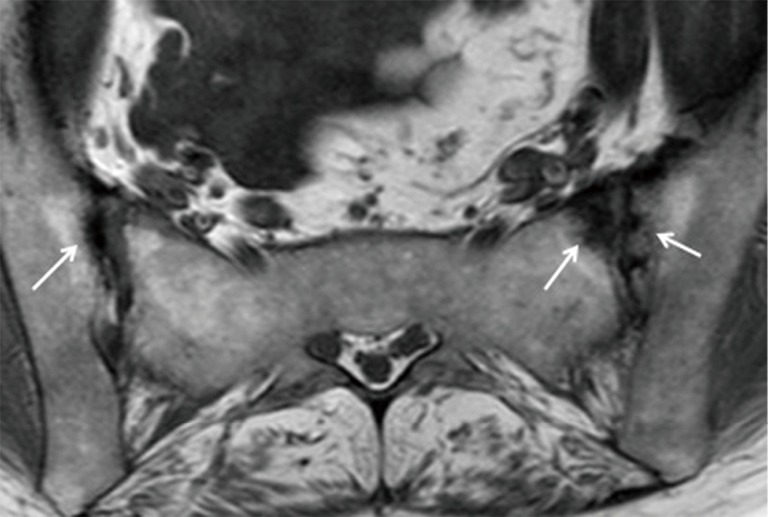
Subchondral sclerosis (arrows) is a non-specific sign of sacroiliitis. Sclerosis can be physiological, related to osteitis condensans ilii, physical stress or osteoarthritis.
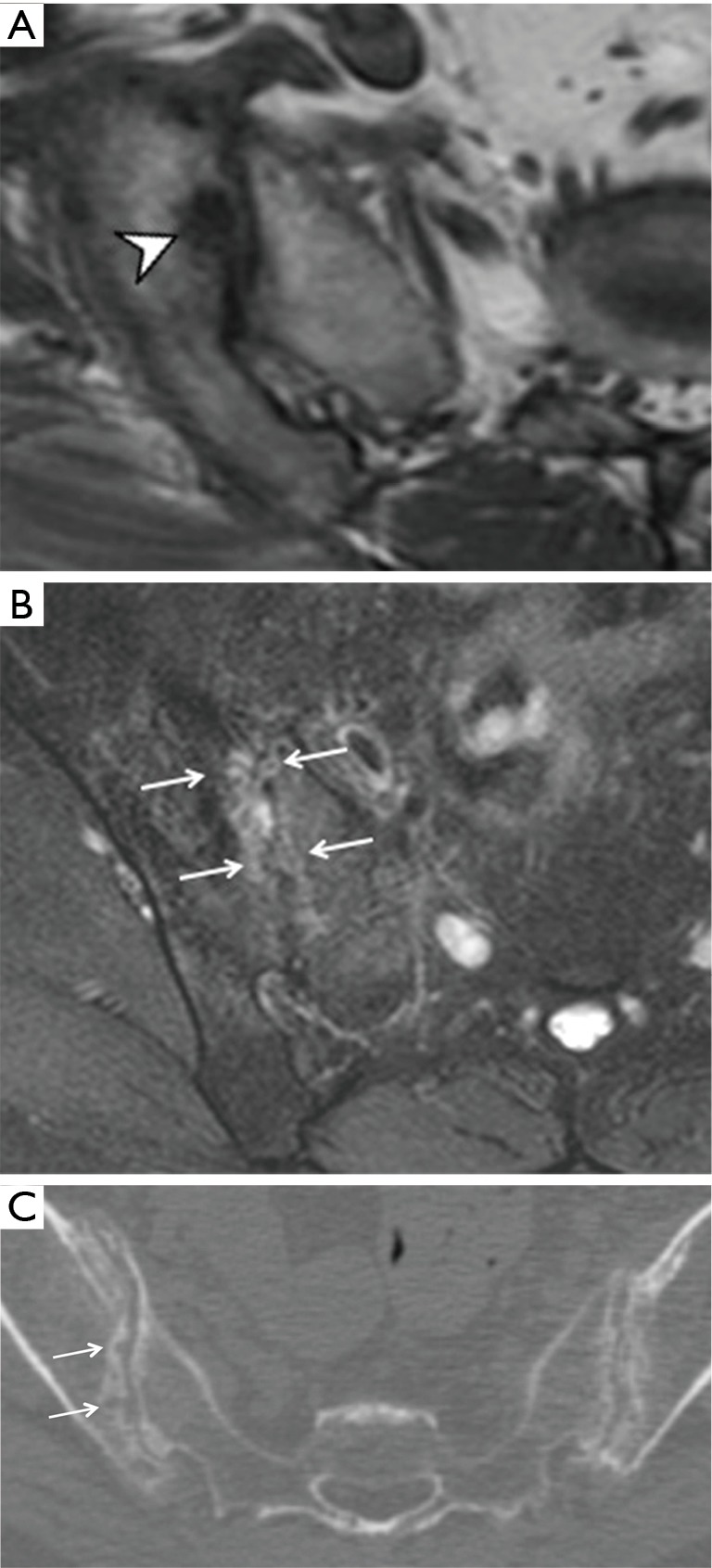
Subchondral erosion can be (A) solitary (arrowhead) or (B) multiple. Multiple coalescent erosions (arrows) can cause widening of the sacroiliac joints giving a “string of pearls” appearance (arrows in C). (C) This is even better demonstrated on CT. Both MRI and CT demonstrate subchondral sclerosis and erosions better than radiographs.
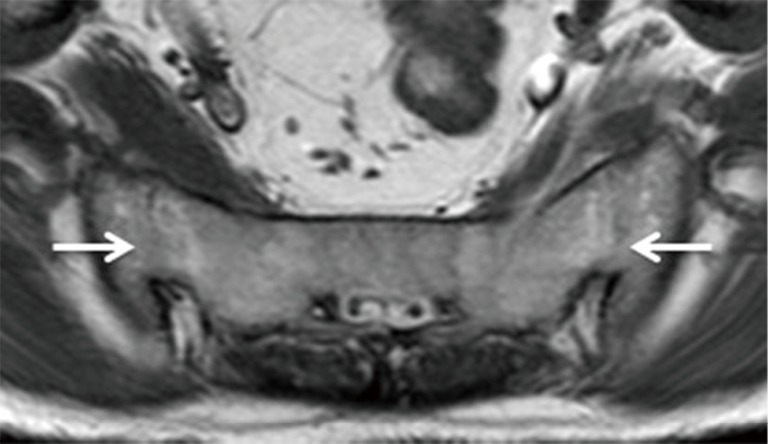
Ankylosis or bony bridging (arrows) can be readily appreciated on MRI. One ideally wants to make the diagnosis of sacroiliitis well before ankylosis becomes apparent.
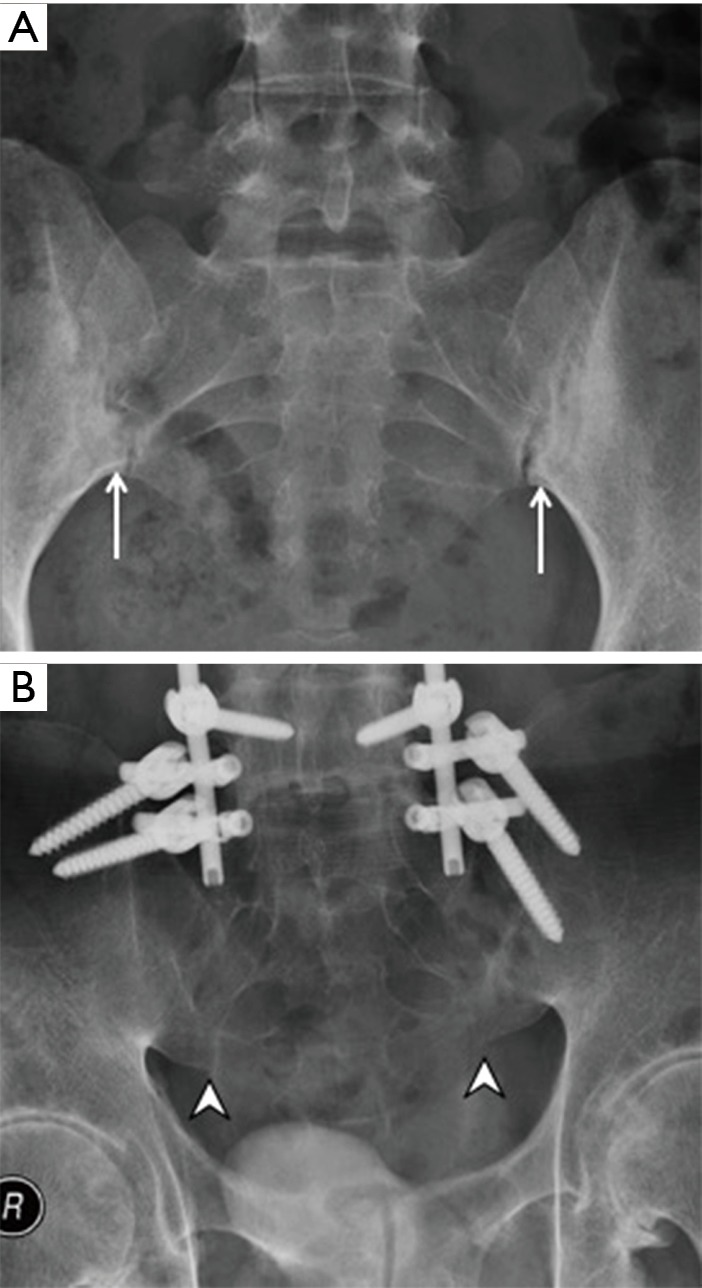
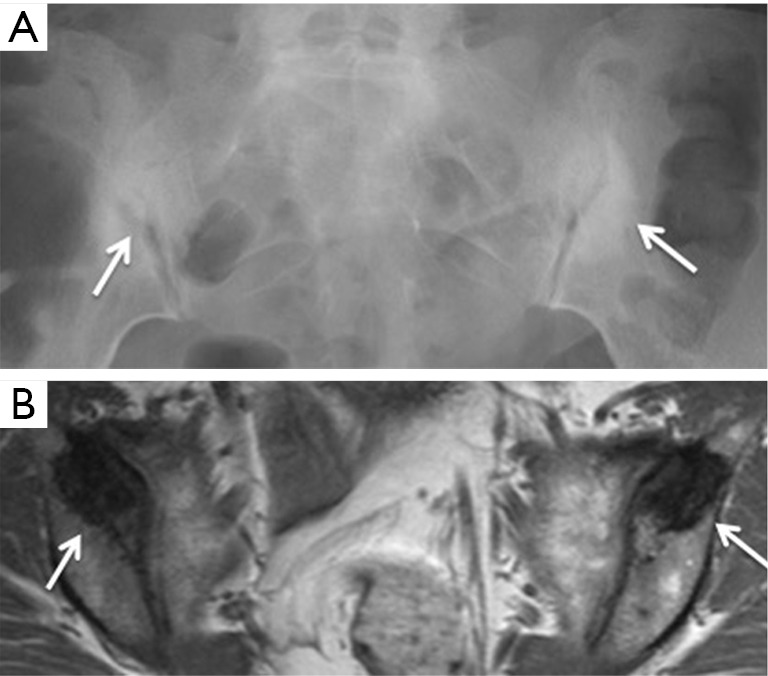
Sacroiliitis. (A) Subchondral sclerosis and erosion (arrows), and (B) ankylosis (arrowheads) of the sacroiliac joints can be appreciated on radiographs. It can take many years before the radiographic changes of sacroiliitis become apparent.
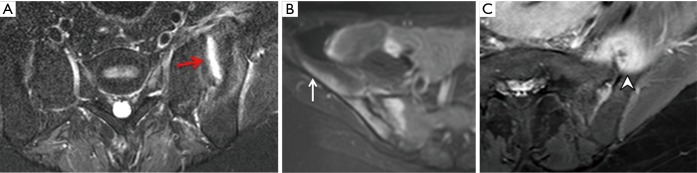
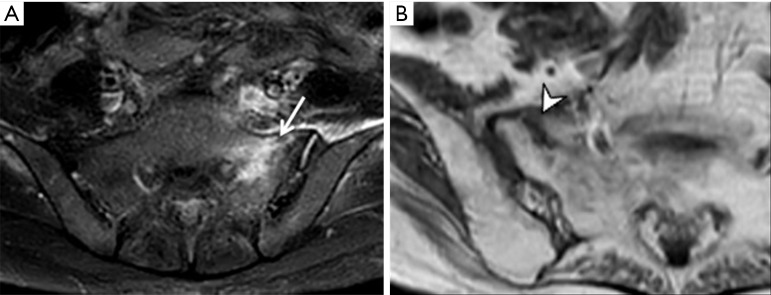
Infective sacroiliitis. (A) Excessive sacroiliac joint fluid (red arrow); (B) inflammation of iliacus muscles (white arrow); and (C) abscess formation (arrowhead) supports the diagnosis of infective sacroiliitis.

Osteoarthritis. (A) Inferior osteophytosis (arrow) on radiograph and (B) anterior marginal osteophytosis (arrowhead) seen on MRI as features of osteoarthritis or instability. (C) Joint irregularity with subchondral sclerosis is due to osteoarthritis rather than sacroiliitis on radiograph.

Stress reaction. Focal patchy oedema (arrow) at the mid-sacral area close to the left sacroiliac joint in a 28-year-old male athlete. No fracture line is evident. The patient recovered with rest.
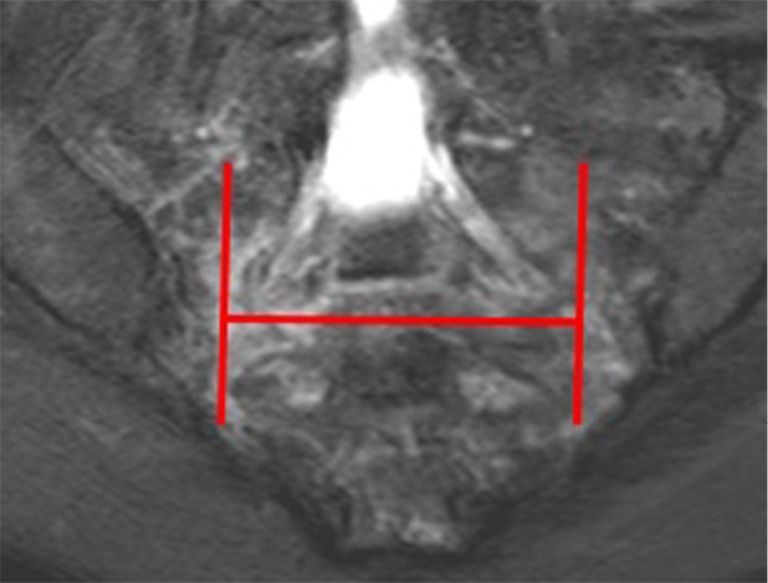
Insufficiency fracture. The fracture line is commonly aligned vertically through the sacral ala and horizontally through the sacral body forming an H-shape which has been termed the “Honda sign”. This sign is classically described on bone scintigraphy, but can be seen on MRI as well.
Reactive stress-related soft tissue changes around the sacroiliac joint. Twenty-seven-year-old professional football player. Radiograph was unremarkable. (A) On MRI, there is severe thickening of the anterior capsule (arrow) on the right side; (B) more proximally, similar though less severe capsular thickening (arrowhead) with osteoarthritis is present on the left side.
Insufficiency fracture. MRI has a very high positive and negative predictive value for insufficiency fracture. It will demonstrate either (A) bone oedema (arrow) ± or (B) a discrete fracture line (arrowhead).
Osteitis condensans ilii (arrows). Well-defined triangular-shaped symmetrical subchondral sclerosis, without erosions or joint space widening at the anterior aspect of the iliac bone on (A) radiograph and (B) MRI.
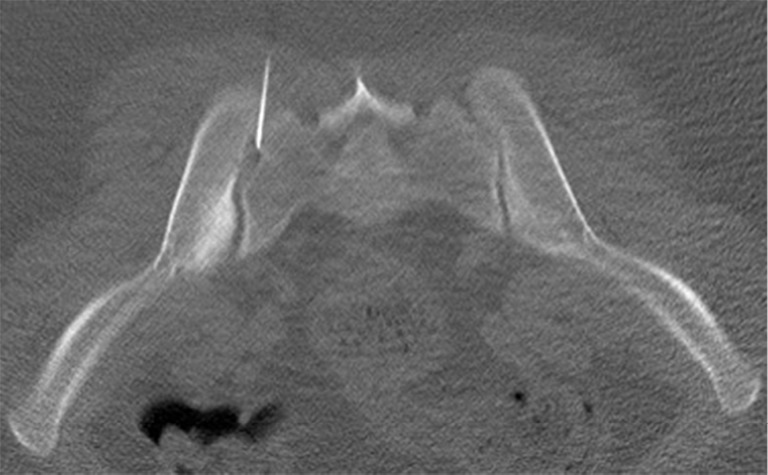
Suspected infective sacroiliitis. Twenty-two-gauge needle insertion into sacroiliac joint for aspiration of joint fluid.

Para-articular bone biopsy to rule out joint infection.
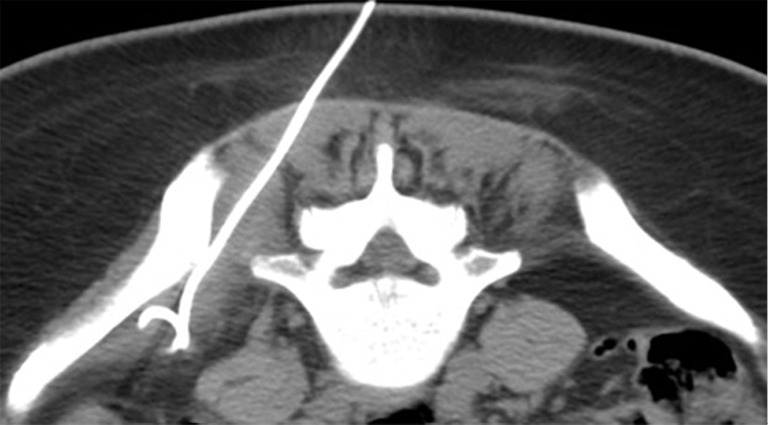
CT-guided pigtail insertion for pigtail drainage of abscess within the iliacus muscle secondary to infective sacroiliitis.

Therapeutic sacroiliac joint injection. This patient has established sacroiliitis with severe joint space narrowing bilaterally. It would be difficult to perform this injection under fluoroscopy or ultrasound guidance. CT-guidance is the method of choice for therapeutic injection.
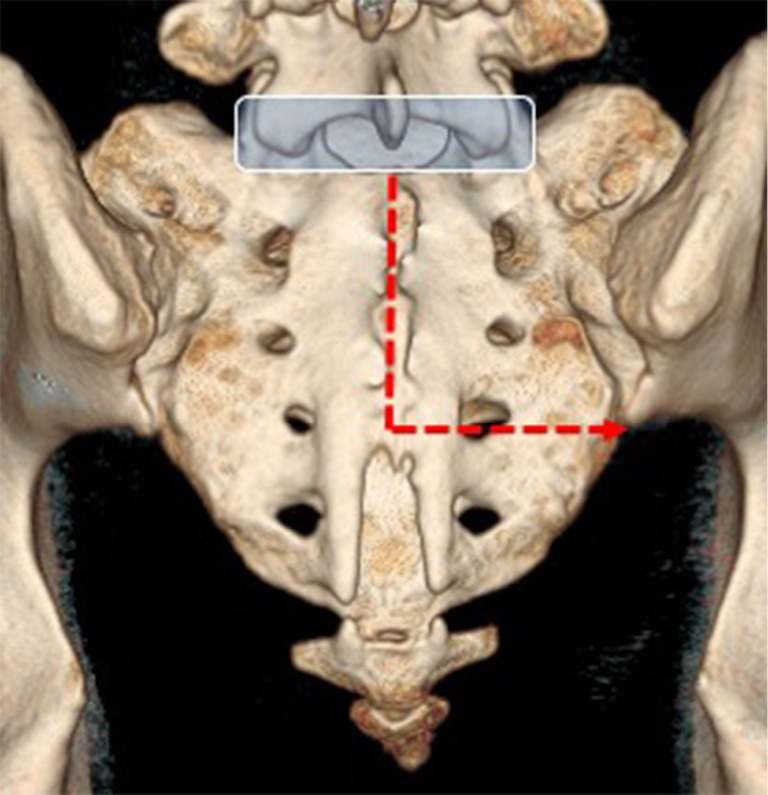
Ultrasound visualization of the sacroiliac joint. The spinous process of L5 is the initial landmark (blue box). On moving the transducer caudally, the hiatus and cornu of the sacrum are seen. The sacroiliac joint can then be seen by moving the transducer first laterally and then proximally towards the inferior margin of the sacroiliac joint
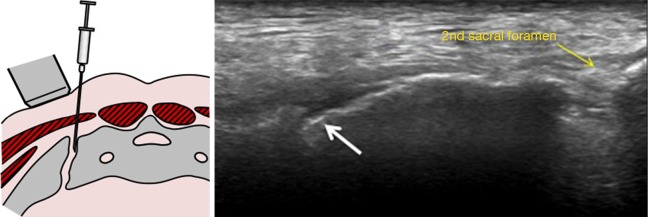
Ultrasound-guided sacroiliac joint (white arrow) injection. Technically, this is feasible, but most of the time the injection is peri-articular rather than intra-articular as the deeper part of the joint cannot be visualized. Ultrasound-guided injection is more suitable for thin patients.

Fluoroscopic-guided sacroiliac joint injection. The patient is positioned prone and is turned oblique until the inferior part of the sacroiliac joint is seen in profile. The distal one-third (red circle) of the joint is targeted for injection.
References
-
- Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos-Vargas R, Dougados M, Hermann KG, Landewé R, Maksymowych W, van der Heijde D. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis 2009;68 Suppl 2:ii1-44. 10.1136/ard.2008.104018 - DOI - PubMed
-
- Peláez-Ballestas I, Navarro-Zarza JE, Julian B, Lopez A, Flores-Camacho R, Casasola-Vargas JC, Sanin LH, Rivas L, Vázquez-Mellado J, Burgos-Vargas R. A community-based study on the prevalence of spondyloarthritis and inflammatory back pain in Mexicans. J Clin Rheumatol 2013;19:57-61. 10.1097/RHU.0b013e3182862e65 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources