

Identification of Candidates for Longer Lung Cancer Screening Intervals Following a Negative Low-Dose Computed Tomography Result
- PMID: 30976808
- PMCID: PMC6748798
- DOI: 10.1093/jnci/djz041
Identification of Candidates for Longer Lung Cancer Screening Intervals Following a Negative Low-Dose Computed Tomography Result
Abstract
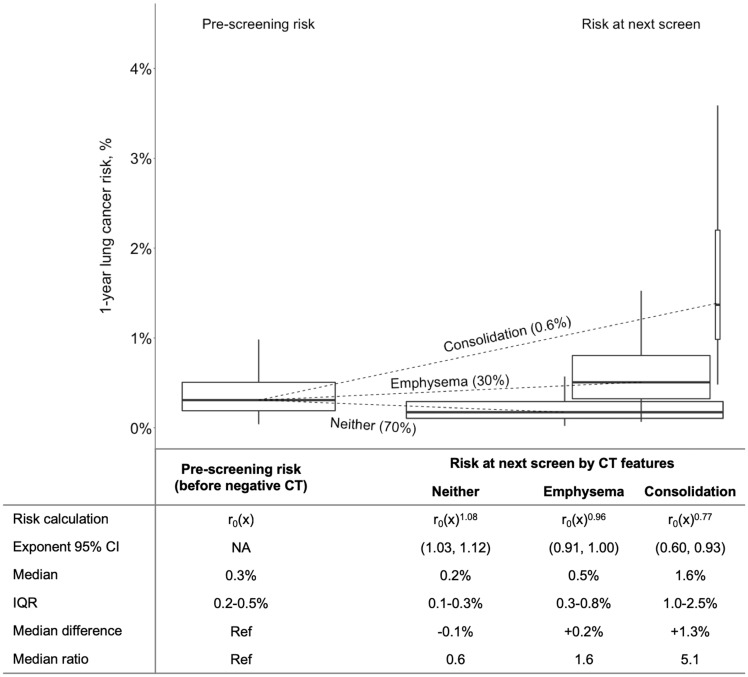
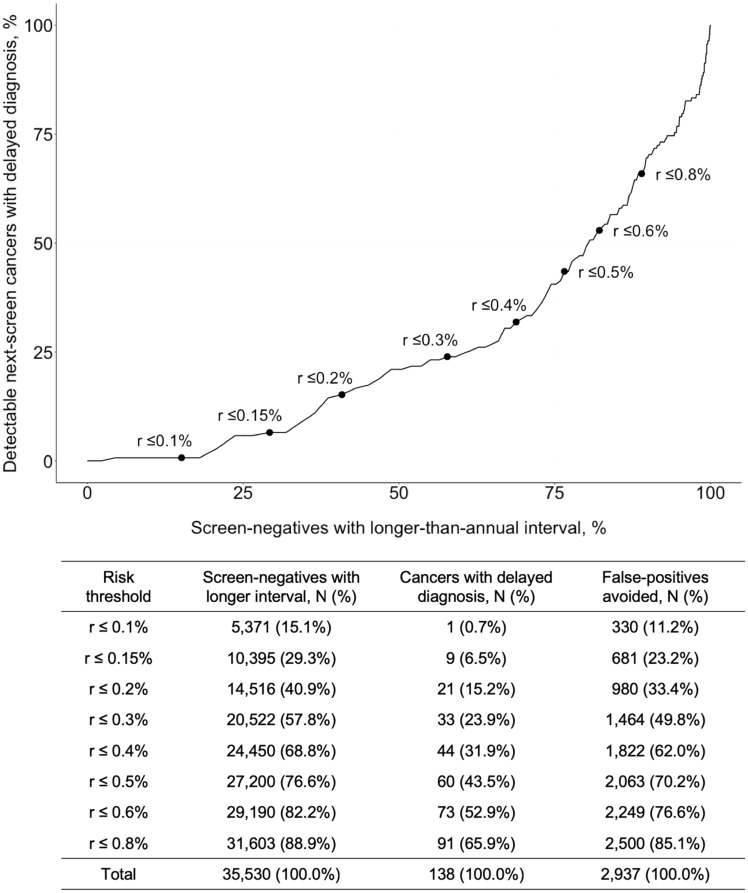
Lengthening the annual low-dose computed tomography (CT) screening interval for individuals at lowest risk of lung cancer could reduce harms and improve efficiency. We analyzed 23 328 participants in the National Lung Screening Trial who had a negative CT screen (no ≥4-mm nodules) to develop an individualized model for lung cancer risk after a negative CT. The Lung Cancer Risk Assessment Tool + CT (LCRAT+CT) updates "prescreening risk" (calculated using traditional risk factors) with selected CT features. At the next annual screen following a negative CT, risk of cancer detection was reduced among the 70% of participants with neither CT-detected emphysema nor consolidation (median risk = 0.2%, interquartile range [IQR] = 0.1%-0.3%). However, risk increased for the 30% with CT emphysema (median risk = 0.5%, IQR = 0.3%-0.8%) and the 0.6% with consolidation (median = 1.6%, IQR = 1.0%-2.5%). As one example, a threshold of next-screen risk lower than 0.3% would lengthen the interval for 57.8% of screen-negatives, thus averting 49.8% of next-screen false-positives among screen-negatives but delaying diagnosis for 23.9% of cancers. Our results support that many, but not all, screen-negatives might reasonably lengthen their CT screening interval.
© World Health Organization, 2019. All rights reserved. The World Health Organization has granted the Publisher permission for the reproduction of this article.
Figures
Comment in
-
Optimal lung cancer screening intervals following a negative low-dose computed tomography result.J Thorac Dis. 2019 Sep;11(Suppl 15):S1916-S1918. doi: 10.21037/jtd.2019.08.85. J Thorac Dis. 2019. PMID: 31632785 Free PMC article. No abstract available.
-
Lung cancer screening: tell me more about post-test risk.J Thorac Dis. 2019 Sep;11(9):3681-3688. doi: 10.21037/jtd.2019.09.28. J Thorac Dis. 2019. PMID: 31656638 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
