Comparison of Laser In Situ Keratomileusis Flap Morphology and Predictability by WaveLight FS200 Femtosecond Laser and Moria Microkeratome: An Anterior Segment Optical Coherence Tomography Study
- PMID: 30977320
- PMCID: PMC6462471
- DOI: 10.3341/kjo.2018.0035
Comparison of Laser In Situ Keratomileusis Flap Morphology and Predictability by WaveLight FS200 Femtosecond Laser and Moria Microkeratome: An Anterior Segment Optical Coherence Tomography Study
Abstract
Purpose: To evaluate laser in situ keratomileusis (LASIK) flap thickness predictability and morphology by femtosecond (FS) laser and microkeratome (MK) using anterior segment optical coherence tomography.
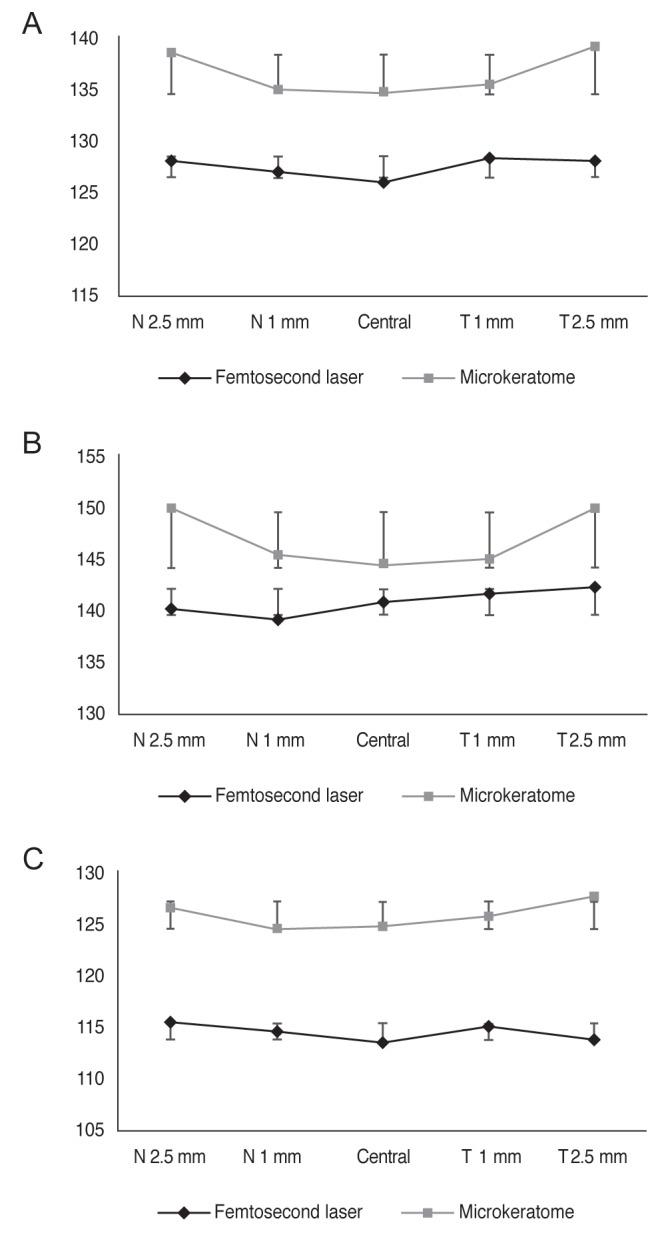
Methods: Fifty-two candidates for the LASIK procedure were stratified into two groups: FS laser-assisted (Allegretto FS-200) and MK flap creation (Moria 2). Flap thickness was determined at five points. The side-cut angle was measured in three directions at the margin interface. LASIK flap assessment was performed one month postoperatively by Spectralis anterior segment optical coherence tomography.
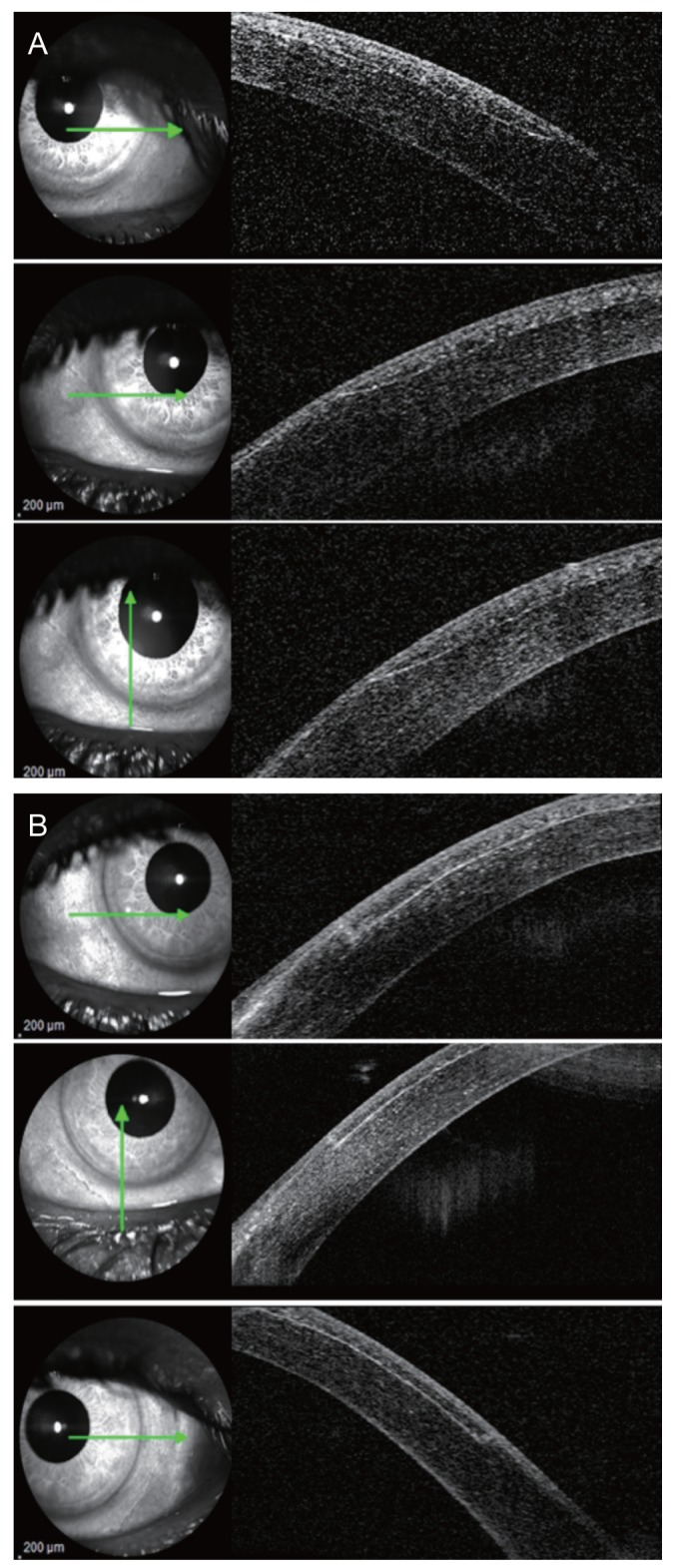
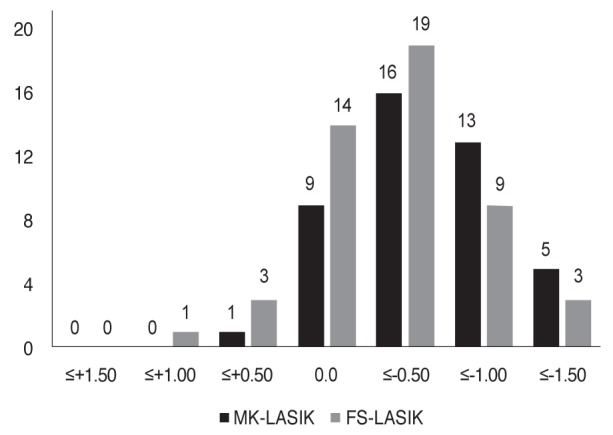
Results: Fifty-two patients (93 eyes) were recruited; 49 eyes were stratified to the FS group and 44 eyes to the MK group. The FS group had relatively even flap configurations, and the MK group had meniscus-shaped flaps. Mean differences between planned and actual flap thickness were 12.93 ± 8.89 and 19.91 ± 5.77 μm in the FS and MK groups, respectively. In thin flaps (100 to 110 μm), there was a significant disparity between the two groups (7.80 ± 4.71 and 19.44 ± 4.46 μm in the FS and MK groups, respectively). However, in thicker flaps (130 μm), comparable flap thickness disparity was achieved (18.54 ± 9.52 and 20.83 ± 5.99 μm in the FS and MK groups, respectively). Mean side-cut angle was 74.29 ± 5.79 degrees and 32.34 ± 4.94 degrees in the FS and MK groups, respectively.
Conclusions: Comparable flap thickness predictability was achieved in thicker flaps (130 μm), while the FS laser technique yielded a more predictable result in thinner flaps (100 to 110 μm). Different flap morphology was observed in meniscus flaps in MK-LASIK and flap morphology in FS-LASIK.
Keywords: Anterior segment optical coherence tomography; Flap morphology; Laser in situ keratomileusis.
© 2019 The Korean Ophthalmological Society.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Sugar A, Rapuano CJ, Culbertson WW, et al. Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy: a report by the American Academy of Ophthalmology. Ophthalmology. 2002;109:175–187. - PubMed
-
- Pietila J, Makinen P, Suominen S, et al. Corneal flap measurements in laser in situ keratomileusis using the Moria M2 automated microkeratome. J Refract Surg. 2005;21:377–385. - PubMed
-
- Knorz MC. Flap and interface complications in LASIK. Curr Opin Ophthalmol. 2002;13:242–245. - PubMed
-
- Ambrosio R, Jr, Wilson SE. Complications of laser in situ keratomileusis: etiology, prevention, and treatment. J Refract Surg. 2001;17:350–379. - PubMed
-
- Kurtz RM, Liu X, Elner VM, et al. Photodisruption in the human cornea as a function of laser pulse width. J Refract Surg. 1997;13:653–658. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical