

Epidemiology of Quick Sequential Organ Failure Assessment Criteria in Undifferentiated Patients and Association With Suspected Infection and Sepsis
- PMID: 30978329
- PMCID: PMC6859245
- DOI: 10.1016/j.chest.2019.03.032
Epidemiology of Quick Sequential Organ Failure Assessment Criteria in Undifferentiated Patients and Association With Suspected Infection and Sepsis
Abstract
Background: The role of Quick Sequential Organ Failure Assessment (qSOFA) criteria in sepsis screening and management is controversial, particularly as they were derived only in patients with suspected infection. We examined the epidemiology and prognostic value of qSOFA in undifferentiated patients.
Methods: We identified patients with ≥ 2 qSOFA criteria within 1 day of admission among all adults admitted to 85 US hospitals from 2012 to 2015 and assessed for suspected infection (using clinical cultures and administration of antibiotics) and sepsis (as defined on the basis of Sepsis-3 criteria). We also examined the discrimination of qSOFA for in-hospital mortality among patients with and without suspected infection, using regression models.
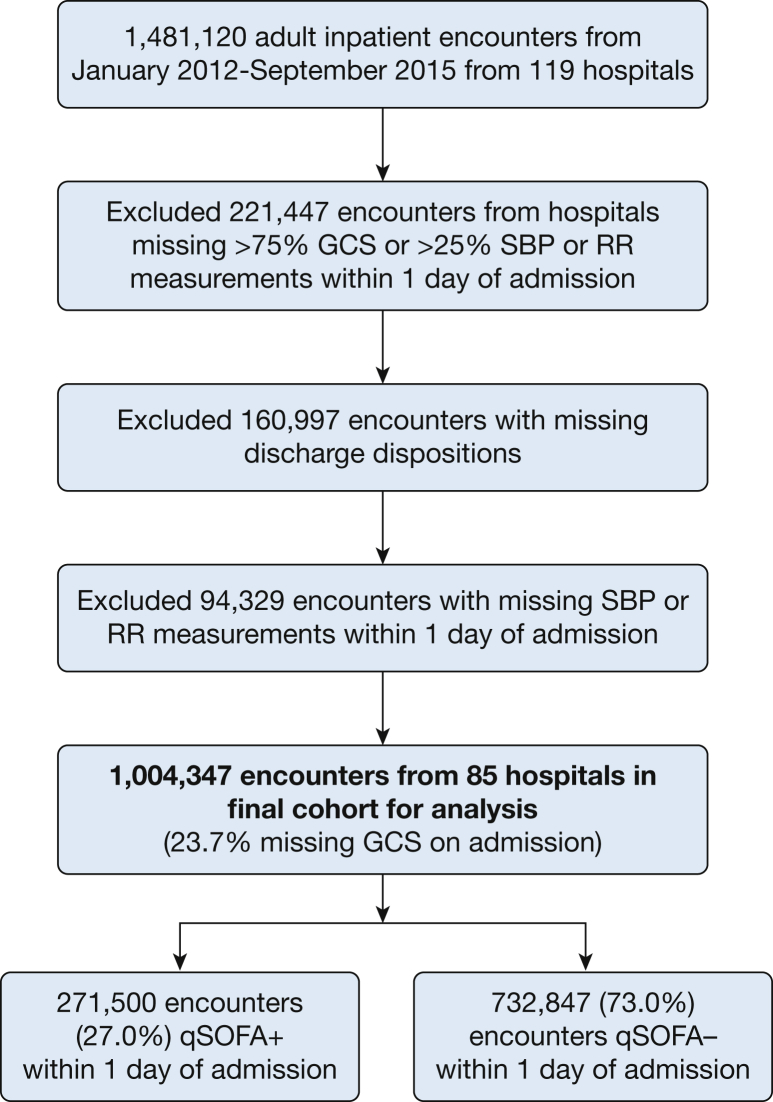
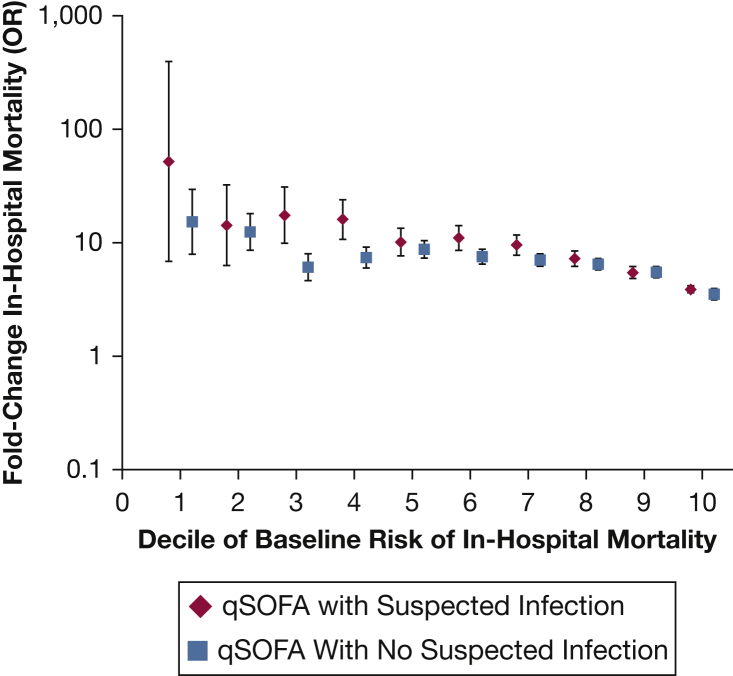
Results: Of 1,004,347 hospitalized patients, 271,500 (27.0%) were qSOFA-positive on admission. Compared with qSOFA-negative patients, qSOFA-positive patients were older (median age, 65 vs 58 years), required ICU admission more often (28.5% vs 6.5%), and had higher mortality (6.7% vs 0.8%) (P < .001 for all comparisons). Sensitivities of qSOFA for suspected infection and sepsis were 41.3% (95% CI, 41.1%-41.5%) and 62.8% (95% CI, 62.4%-63.1%), respectively; positive predictive values were 31.0% (95% CI, 30.8%-31.1%) and 17.4% (95% CI, 17.2%-17.5%). The area under the receiver operating characteristic curve for mortality was lower for qSOFA in patients with suspected infection vs those without (0.814 vs 0.875; P < .001).
Conclusions: Only one in three patients who are qSOFA-positive on admission has suspected infection, and one in six has sepsis. qSOFA also has low sensitivity for identifying suspected infection and sepsis, and its prognostic significance is not specific to infection. More sensitive and specific tools for sepsis screening and risk stratification are needed.
Keywords: epidemiology; infection; organ function/dysfunction; qSOFA; sepsis.
Copyright © 2019 American College of Chest Physicians. All rights reserved.
Figures
Comment in
-
Quick Sequential Organ Failure Assessment Is Not Good for Ruling Sepsis In or Out.Chest. 2019 Aug;156(2):197-199. doi: 10.1016/j.chest.2019.06.003. Chest. 2019. PMID: 31395253 No abstract available.
-
Response.Chest. 2020 Jan;157(1):231-232. doi: 10.1016/j.chest.2019.09.010. Chest. 2020. PMID: 31916956 No abstract available.
-
Can qSOFA Perform Better If Combined With Frailty Measures in Elderly Patients?Chest. 2020 Jan;157(1):231. doi: 10.1016/j.chest.2019.09.011. Chest. 2020. PMID: 31916957 No abstract available.
-
Dear qSOFA, We Would Like to Get to Know You Better….Chest. 2020 Jan;157(1):232-233. doi: 10.1016/j.chest.2019.09.013. Chest. 2020. PMID: 31916958 No abstract available.
-
Response.Chest. 2020 Jan;157(1):233-234. doi: 10.1016/j.chest.2019.09.014. Chest. 2020. PMID: 31916959 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
