

Combining activatable nanodelivery with immunotherapy in a murine breast cancer model
- PMID: 30978432
- PMCID: PMC6660242
- DOI: 10.1016/j.jconrel.2019.04.008
Combining activatable nanodelivery with immunotherapy in a murine breast cancer model
Abstract
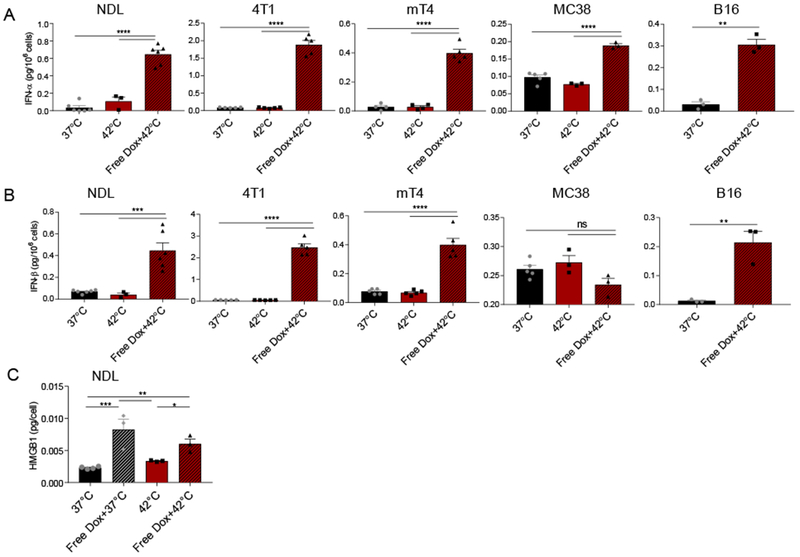
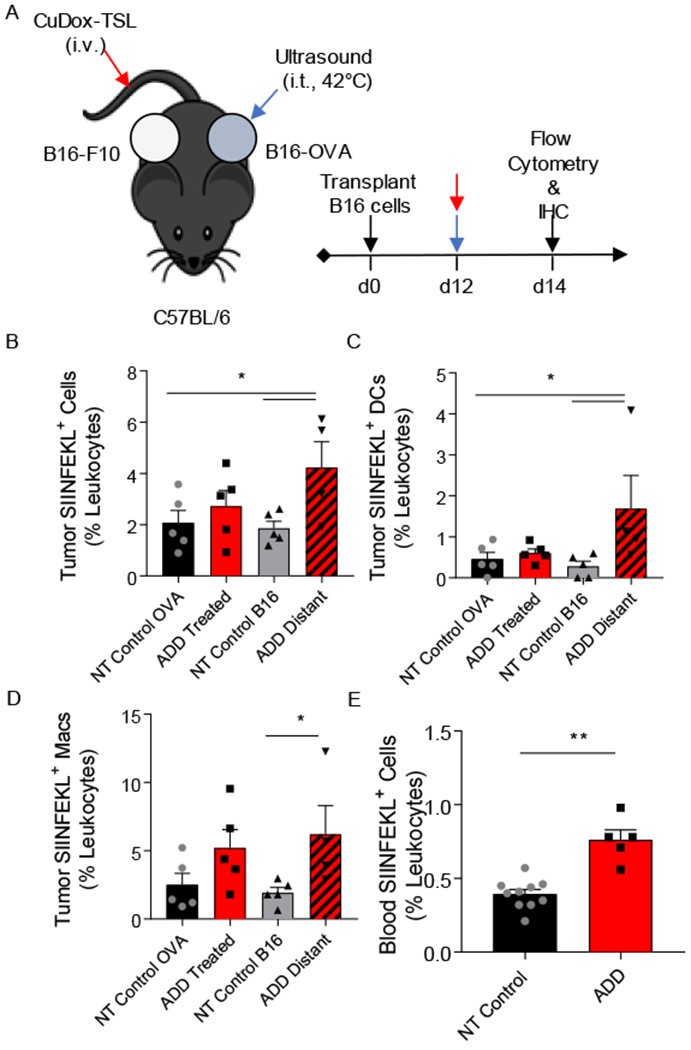
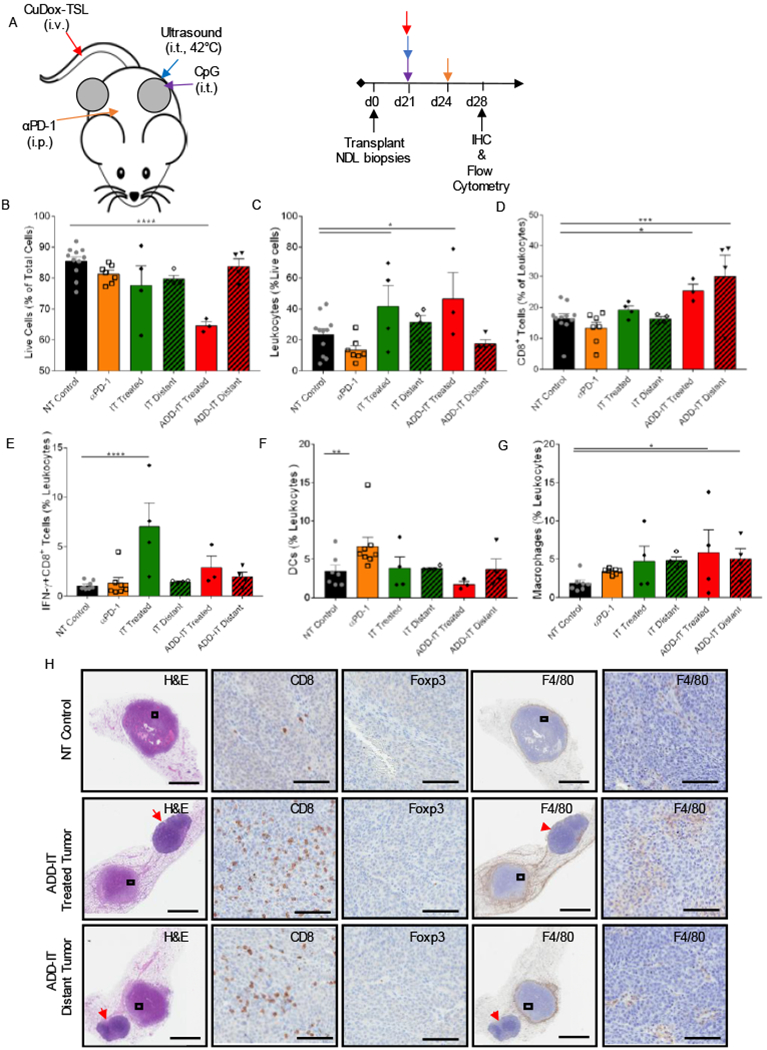
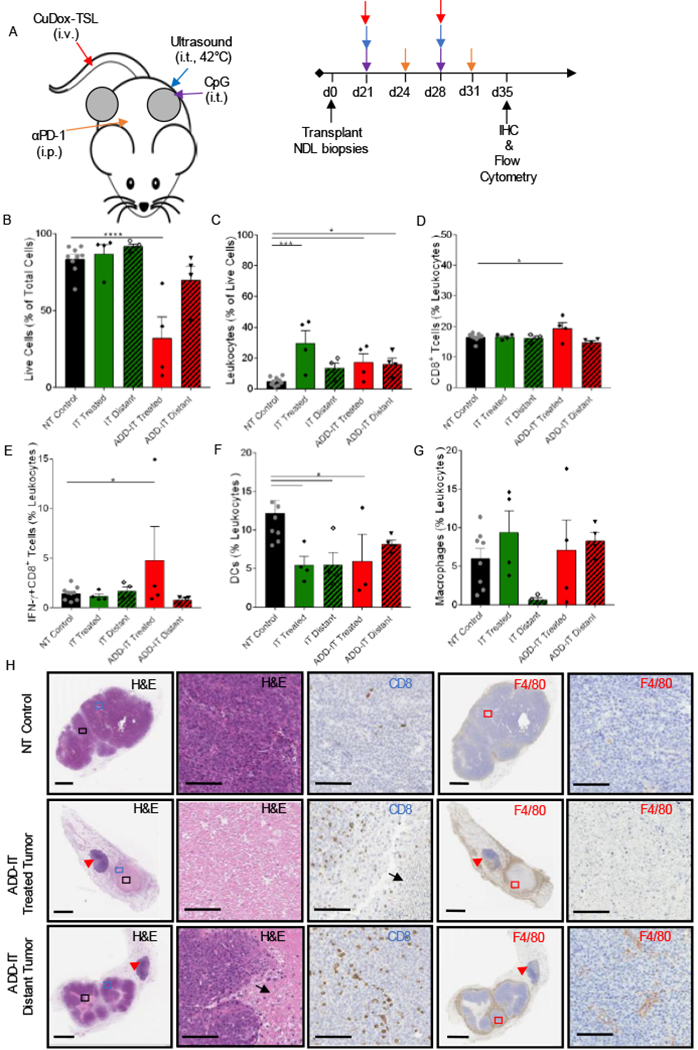
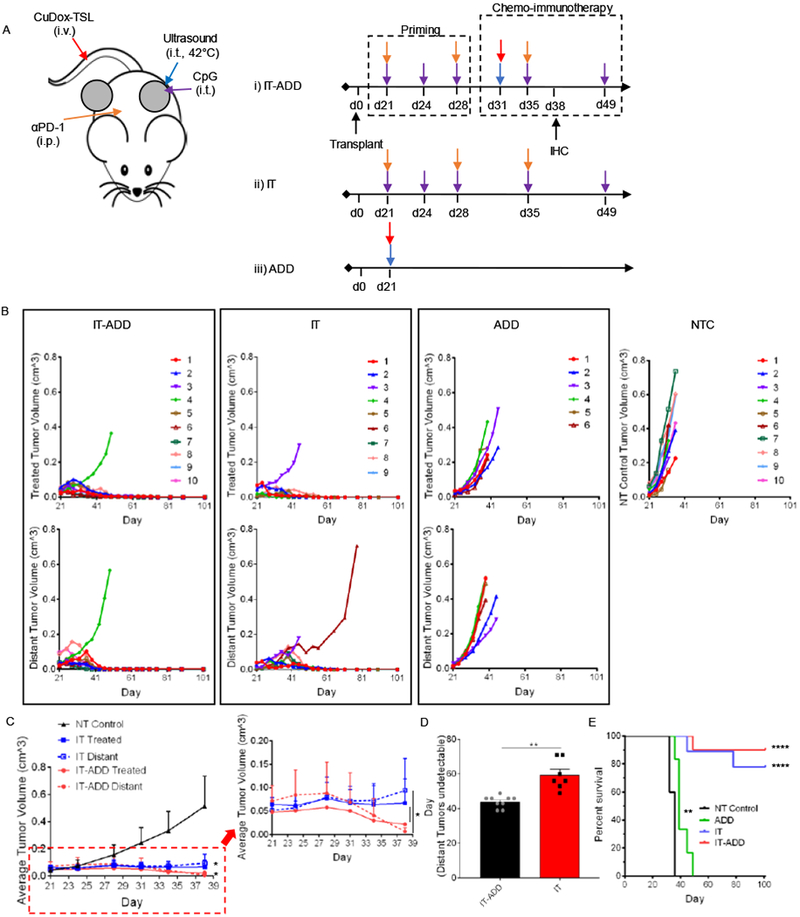
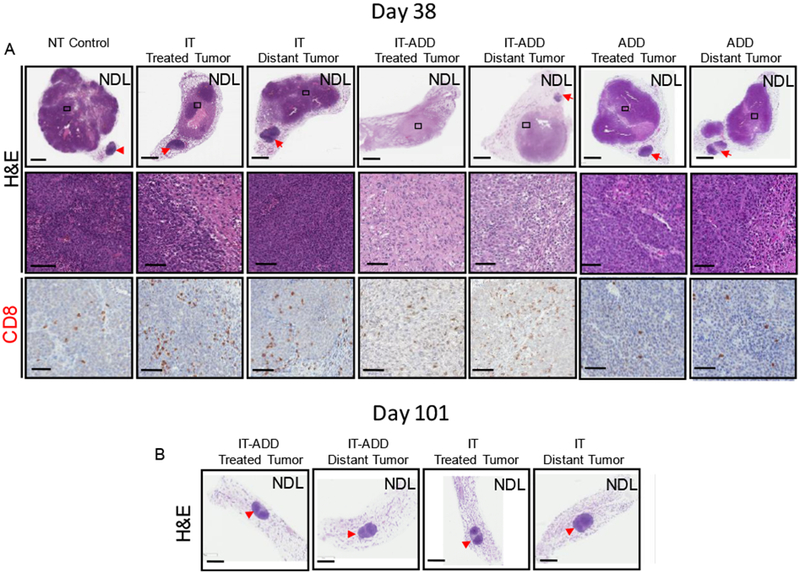
A successful chemotherapy-immunotherapy solid-tumor protocol should accomplish the following goals: debulk large tumors, release tumor antigen for cross-presentation and cross-priming, release cancer-suppressive cytokines and enhance anti-tumor immune cell populations. Thermally-activated drug delivery particles have the potential to synergize with immunotherapeutics to accomplish these goals; activation can release chemotherapy within bulky solid tumors and can enhance response when combined with immunotherapy. We set out to determine whether a single protocol, combining locally-activated chemotherapy and agonist immunotherapy, could accomplish these goals and yield a potentially translational therapy. For effective delivery of free doxorubicin to tumors with minimal toxicity, we stabilized doxorubicin with copper in temperature-sensitive liposomes that rapidly release free drug in the vasculature of cancer lesions upon exposure to ultrasound-mediated hyperthermia. We found that in vitro exposure of tumor cells to hyperthermia and doxorubicin resulted in immunogenic cell death and the local release of type I interferons across murine cancer cell lines. Following intravenous injection, local activation of the liposomes within a single tumor released doxorubicin and enhanced cross-presentation of a model antigen at distant tumor sites. While a variety of protocols achieved a complete response in >50% of treated mice, the complete response rate was greatest (90%) when 1 week of immunotherapy priming preceded a single activatable chemotherapeutic administration. While repeated chemotherapeutic delivery reduced local viable tumor, the complete response rate and a subset of tumor immune cells were also reduced. Taken together, the results suggest that activatable chemotherapy can enhance adjuvant immunotherapy; however, in a murine model the systemic adaptive immune response was greatest with a single administration of chemotherapy.
Keywords: Breast cancer; CpG; Doxorubicin; Immunotherapy; Temperature-sensitive liposome; Ultrasound; αPD-1.
Copyright © 2019 Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest
The authors declare no completing financial of interest.
Figures
References
-
- Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, Lee W, Yuan J, Wong P, Ho TS, Miller ML, Rekhtman N, Moreira AL, Ibrahim F, Bruggeman C, Gasmi B, Zappasodi R, Maeda Y, Sander C, Garon EB, Merghoub T, Wolchok JD, Schumacher TN, Chan TA, Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer, Science. 348 (2015) 124–128. doi:10.1126/science.aaa1348. - DOI - PMC - PubMed
-
- Van Allen EM, Miao D, Schilling B, Shukla SA, Blank C, Zimmer L, Sucker A, Hillen U, Foppen MHG, Goldinger SM, Utikal J, Hassel JC, Weide B, Kaehler KC, Loquai C, Mohr P, Gutzmer R, Dummer R, Gabriel S, Wu CJ, Schadendorf D, Garraway LA, Genomic correlates of response to CTLA-4 blockade in metastatic melanoma, Science. 350 (2015) 207–211. doi:10.1126/science.aad0095. - DOI - PMC - PubMed
-
- McGranahan N, Furness AJ, Rosenthal R, Ramskov S, Lyngaa R, Saini SK, Jamal-Hanjani M, Wilson GA, Birkbak NJ, Hiley CT, Watkins TB, Shafi S, Murugaesu N, Mitter R, Akarca AU, Linares J, Marafioti T, Henry JY, Van Allen EM, Miao D, Schilling B, Schadendorf D, Garraway LA, Makarov V, Rizvi NA, Snyder A, Hellmann MD, Merghoub T, Wolchok JD, Shukla SA, Wu CJ, Peggs KS, Chan TA, Hadrup SR, Quezada SA, Swanton C, Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade, Science. 351 (2016) 1463–1469. doi:10.1126/science.aaf1490. - DOI - PMC - PubMed
