

ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis
- PMID: 30979521
- PMCID: PMC8594622
- DOI: 10.1016/j.gie.2018.10.001
ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis
Abstract
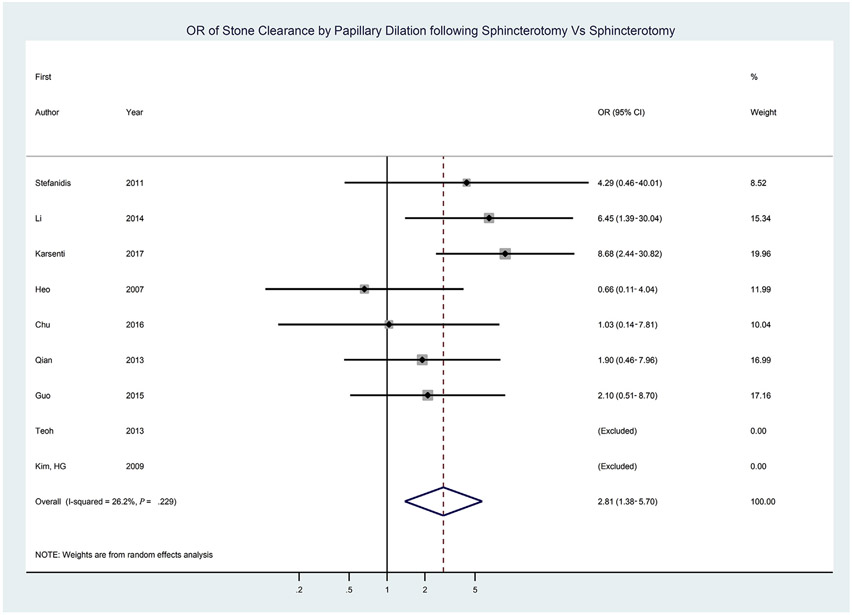
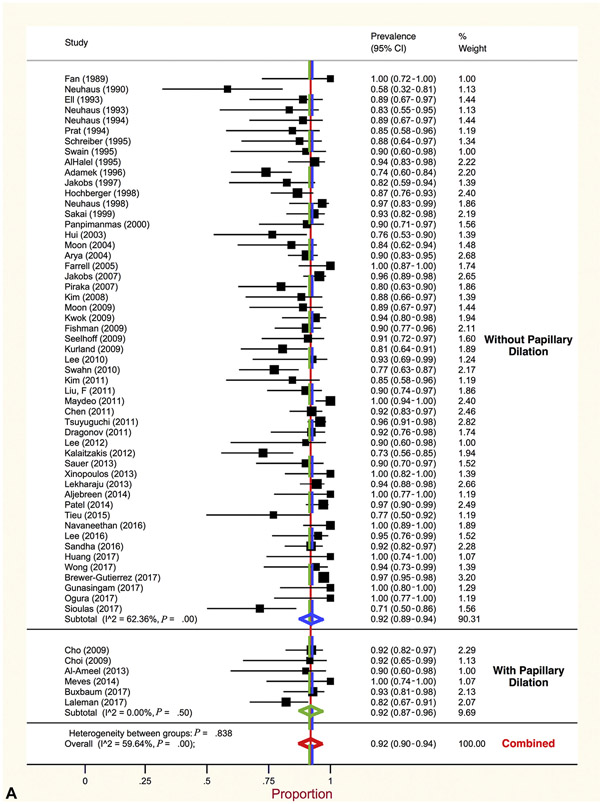
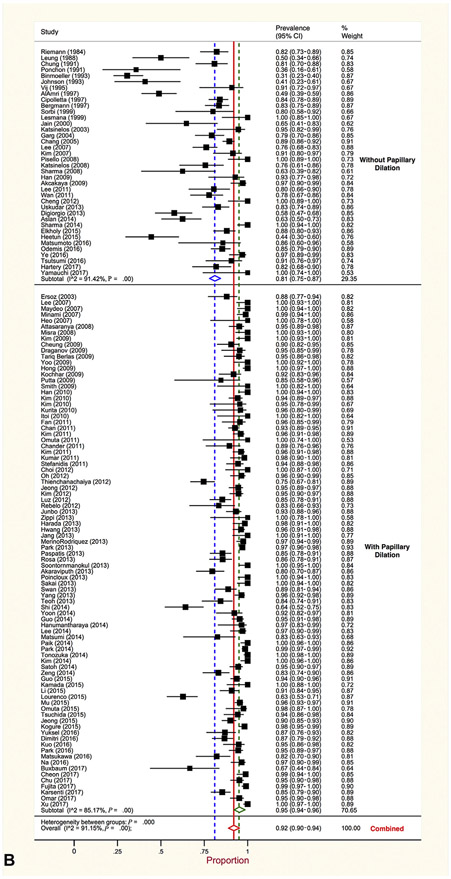
Each year choledocholithiasis results in biliary obstruction, cholangitis, and pancreatitis in a significant number of patients. The primary treatment, ERCP, is minimally invasive but associated with adverse events in 6% to 15%. This American Society for Gastrointestinal Endoscopy (ASGE) Standard of Practice (SOP) Guideline provides evidence-based recommendations for the endoscopic evaluation and treatment of choledocholithiasis. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was used to rigorously review and synthesize the contemporary literature regarding the following topics: EUS versus MRCP for diagnosis, the role of early ERCP in gallstone pancreatitis, endoscopic papillary dilation after sphincterotomy versus sphincterotomy alone for large bile duct stones, and impact of ERCP-guided intraductal therapy for large and difficult choledocholithiasis. Comprehensive systematic reviews were also performed to assess the following: same-admission cholecystectomy for gallstone pancreatitis, clinical predictors of choledocholithiasis, optimal timing of ERCP vis-à-vis cholecystectomy, management of Mirizzi syndrome and hepatolithiasis, and biliary stent therapy for choledocholithiasis. Core clinical questions were derived using an iterative process by the ASGE SOP Committee. This body developed all recommendations founded on the certainty of the evidence, balance of risks and harms, consideration of stakeholder preferences, resource utilization, and cost-effectiveness.
Copyright © 2019. Published by Elsevier Inc.
Figures
References
-
- Paumgartner G, Sauerbruch T. Gallstones: pathogenesis. Lancet 1991;338:1117–21. - PubMed
-
- Hall MJ, Schwartzman A, Zhang J, et al. Ambulatory surgery data from hospitals and ambulatory surgery centers: United States, 2010. National Health Statistics Reports; 2017. Available at: https://www.cdc.gov/nchs/data/nhsr/nhsr102.pdf. - PubMed
-
- Frossard JL, Morel PM. Detection and management of bile duct stones. Gastrointest Endosc 2010;72:808–16. - PubMed
-
- Sun SX, Kulaylat AN, Hollenbeak CS, et al. Cost-effective decisions in detecting silent common bile duct gallstones during laparoscopic cholecystectomy. Ann Surg 2016;263:1164–72. - PubMed
