

Immunoreactivity for prostate specific antigen and Ki67 differentiates subgroups of prostate cancer related to outcome
- PMID: 30980038
- PMCID: PMC6760646
- DOI: 10.1038/s41379-019-0260-6
Immunoreactivity for prostate specific antigen and Ki67 differentiates subgroups of prostate cancer related to outcome
Abstract
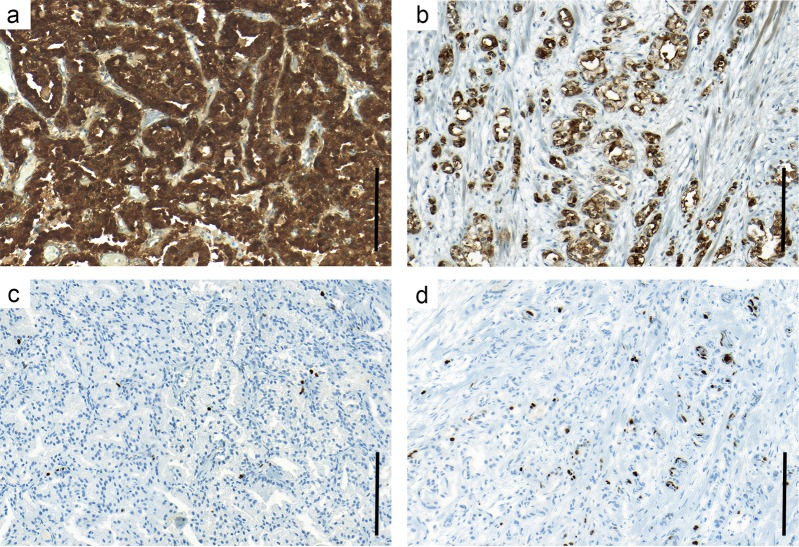
Based on gene-expression profiles, prostate tumors can be subdivided into subtypes with different aggressiveness and response to treatment. We investigated if similar clinically relevant subgroups can be identified simply by the combination of two immunohistochemistry markers: one for tumor cell differentiation (prostate specific antigen, PSA) and one for proliferation (Ki67). This was analyzed in men with prostate cancer diagnosed at transurethral resection of the prostate 1975-1991 (n = 331) where the majority was managed by watchful waiting. Ki67 and PSA immunoreactivity was related to outcome and to tumor characteristics previously associated with prognosis. Increased Ki67 and decreased PSA were associated with poor outcome, and they provided independent prognostic information from Gleason score. A combinatory score for PSA and Ki67 immunoreactivity was produced using the median PSA and Ki67 levels as cut-off (for Ki67 the upper quartile was also evaluated) for differentiation into subgroups. Patients with PSA low/Ki67 high tumors showed higher Gleason score, more advanced tumor stage, and higher risk of prostate cancer death compared to other patients. Their tumor epithelial cells were often ERG positive and expressed higher levels of ErbB2, phosphorylated epidermal growth factor receptor (pEGF-R) and protein kinase B (pAkt), and their tumor stroma showed a reactive response with type 2 macrophage infiltration, high density of blood vessels and hyaluronic acid, and with reduced levels of caveolin-1, androgen receptors, and mast cells. In contrast, men with PSA high/Ki67 low tumors were characterized by low Gleason score, and the most favorable outcome amongst PSA/Ki67-defined subgroups. Men with PSA low/Ki67 low tumors showed clinical and tumor characteristics intermediate of the two groups above. A combinatory PSA/Ki67 immunoreactivity score identifies subgroups of prostate cancers with different epithelial and stroma phenotypes and highly different outcome but the clinical usefulness of this approach needs to be validated in other cohorts.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Ylitalo EB, Thysell E, Jernberg E, Lundholm M, Crnalic S, Egevad L, et al. Subgroups of castration-resistant prostate cancer bone metastases defined through an inverse relationship between androgen receptor activity and immune response. Eur Urol. 2017;71:776–787. doi: 10.1016/j.eururo.2016.07.033. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
