

Adrenocortical carcinoma: presentation and outcome of a contemporary patient series
- PMID: 30980285
- PMCID: PMC6606857
- DOI: 10.1007/s12020-019-01918-9
Adrenocortical carcinoma: presentation and outcome of a contemporary patient series
Abstract
Background: Adrenocortical carcinoma (ACC) is a rare endocrine carcinoma with poor 5-year survival rates of < 40%. According to the literature, ACC is rarely an incidental imaging finding. However, presentation, treatment and outcome may differ in modern series.
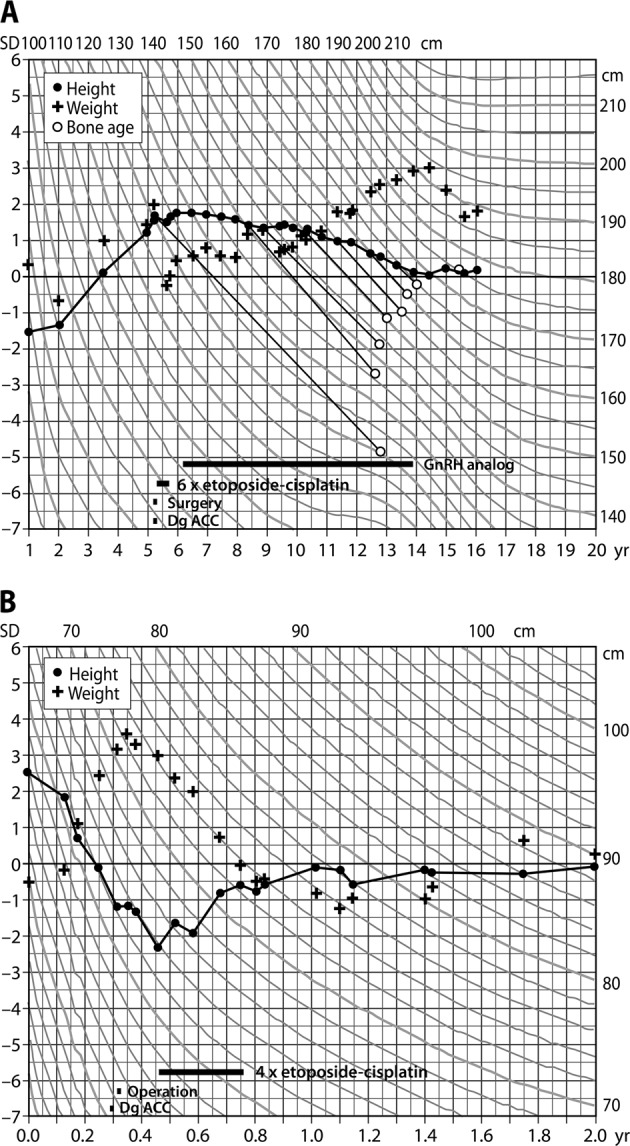
Design and methods: We studied all patients (n = 47, four children) from a single centre during years 2002-2018. We re-evaluated radiologic and histopathological findings and assessed treatments and outcome. We searched for possible TP53 gene defects and assessed nationwide incidence of ACC.
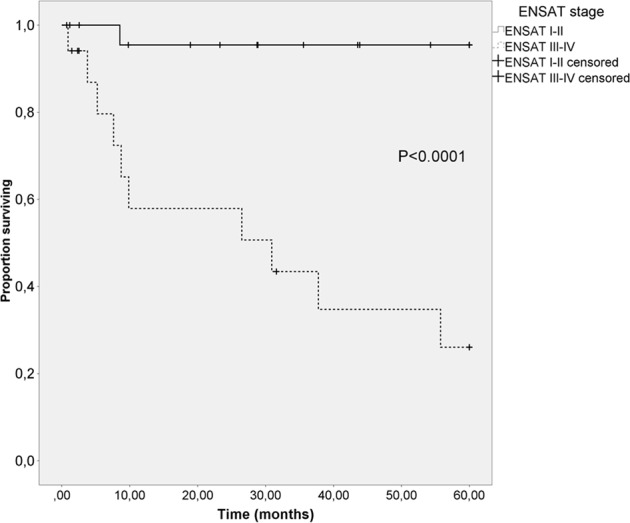
Results: In adults, incidental radiologic finding led to diagnosis in 79% at median age of 61 years. ENSAT stage I, II, III and IV was 19%, 40%, 19% and 21%, respectively. Nonenhanced CT demonstrated > 20 Hounsfield Units (HU) for all tumours (median 34 (21-45)), median size 92 mm (20-196), Ki67 17% (1-40%), Weiss score 7 (4-9) and Helsinki score 24 (4-48). ACC was more often found in the left than the right adrenal (p < 0.05). One child had Beckwith-Wiedemann and one a TP53 mutation. In adults, the primary tumour was resected in 88 and 79% received adjuvant mitotane therapy. Median hospital stay was significantly shorter in the laparoscopic vs. open surgery group (4 (3-7) vs. 8 (5-38) days, respectively; p < 0.001). In 3/4 patients, prolonged remission of > 5 to > 10 years was achieved after repeated surgery of metastases. Overall 5-year survival was 67%, and 96% vs. 26% for ENSAT stage I-II vs. III-IV (p < 0.0001). ENSAT stage and Ki67 predicted survival, type of surgery did not. Mitotane associated with better survival.
Conclusions: Contemporary ACC predominantly presents as an incidental imaging finding, characterised by HU > 20 on nonenhanced CT but variable tumour size (20-196 mm). Malignancy cannot be ruled out by small tumour size only. The 5-year survival of 96% in ENSAT stage I-III compares favourably to previous studies.
Keywords: Adrenocortical carcinoma; Complications; ENSAT stage; Hounsfield units; Mitotane; Surgery; Survival.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Kerkhofs TM, Verhoeven RH, Van der Zwan JM, Dieleman J, Kerstens MN, Links TP, Van de Poll-Franse LV, Haak HR. Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. Eur. J. Cancer. 2013;49:2579–2586. doi: 10.1016/j.ejca.2013.02.034. - DOI - PubMed
-
- Fassnacht M, Johanssen S, Quinkler M, Bucsky P, Willenberg HS, Beuschlein F, Terzolo M, Mueller HH, Hahner S, Allolio B, German Adrenocortical Carcinoma Registry Group, European Network for the Study of Adrenal Tumors Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: proposal for a Revised TNM Classification. Cancer. 2009;115:243–250. doi: 10.1002/cncr.24030. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
