

First-line treatment of essential hypertension: A real-world analysis across four antihypertensive treatment classes
- PMID: 30980608
- PMCID: PMC8030363
- DOI: 10.1111/jch.13531
First-line treatment of essential hypertension: A real-world analysis across four antihypertensive treatment classes
Abstract
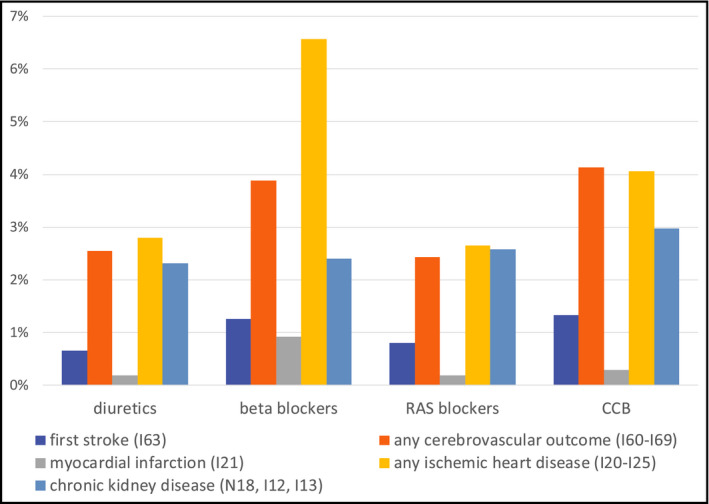
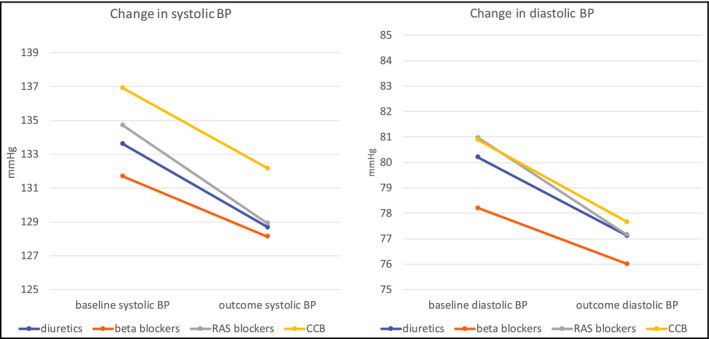
The relative efficacy of antihypertensive treatment has been assessed primarily by randomized clinical trials (RCTs). The increasing availability of electronic medical records (EMR) allows results from RCT to be compared to data from actual clinical practice. EMR from TriNetX were used to compare patients starting and adhering to antihypertensive treatment on diuretics, beta blockers, angiotensin II or ACE inhibitors, or calcium channel blockers for at least 36 months. Cardiovascular (CV) events as defined by ICD-10 codes were evaluated for an observation period of three years. Outcomes were assessed with and without propensity score matching for confounding factors. A total of 79 288 patients fulfilled the criteria for first-line therapy and adherence (17.4% diuretics, 25.9% beta blockers, 45.1% inhibitors of the renin-angiotensin system, and 11.6% calcium channel blockers). Differences in demography and comorbidities were consistent with expectations based on treatment guidelines. RAS blockers showed the best BP control (28.7% episodes of uncontrolled BP) and, together with diuretics, the lowest rate of CV events (diuretics, 5.2%; RAS blockers, 5.4%). Beta blockers were associated with the highest rate of uncontrolled BP (45.9%) and a high CV event rate (9.5%). These trends remained after matching the cohorts for confounding factors. EMR show that actual prescribing behavior for first-line treatment of essential hypertension reflects treatment guidelines. Patients taking either RAS blockers or diuretics experienced the lowest CV event rates. Beta blockers, even when adjusted for pre-existing cardiovascular conditions, do not seem to be as protective against CV events as the three other classes.
Keywords: first-line treatment; hypertension; monotherapy; real-world data.
©2019 Wiley Periodicals, Inc.
Conflict of interest statement
MS is Chief Medical Officer of TriNetX Inc, the data network and analytics platform used for this publication. SH was employee of TriNetX at the time of analysis and manuscript preparation. MS owns stocks from Merck and Allergan, stemming from previous employments. Neither of these, nor any other pharmaceutical company was involved or had any influence in the design of the study; the collection, analysis, and interpretation of data; writing of the report; or the decision to submit the report for publication.
Figures
References
-
- Benjamin EJ, Nasir K, Virani SS, et al. Heart disease and stroke statistics—2018 Update. Circulation. 2018;137:e67‐e492. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. JACC. 2018;71:e127‐248. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
