

Cost-Effectiveness of Colonoscopy-Based Colorectal Cancer Screening in Childhood Cancer Survivors
- PMID: 30980665
- PMCID: PMC6855986
- DOI: 10.1093/jnci/djz060
Cost-Effectiveness of Colonoscopy-Based Colorectal Cancer Screening in Childhood Cancer Survivors
Abstract
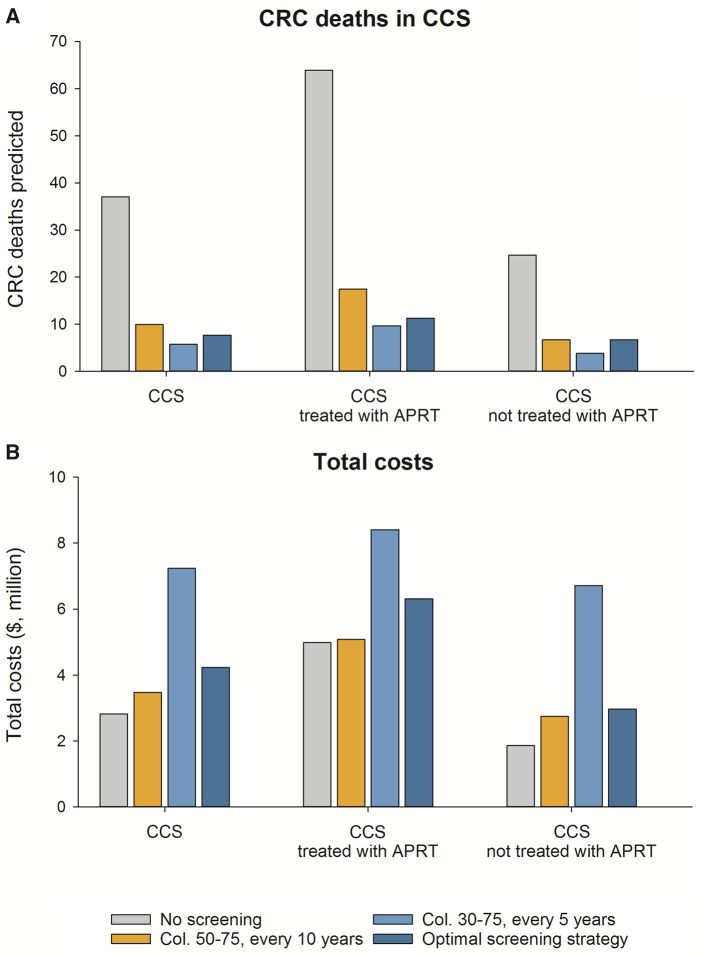
Background: Childhood cancer survivors (CCS) are at increased risk of developing colorectal cancer (CRC) compared to the general population, especially those previously exposed to abdominal or pelvic radiation therapy (APRT). However, the benefits and costs of CRC screening in CCS are unclear. In this study, we evaluated the cost-effectiveness of early-initiated colonoscopy screening in CCS.
Methods: We adjusted a previously validated model of CRC screening in the US population (MISCAN-Colon) to reflect CRC and other-cause mortality risk in CCS. We evaluated 91 colonoscopy screening strategies varying in screening interval, age to start, and age to stop screening for all CCS combined and for those treated with or without APRT. Primary outcomes were CRC deaths averted (compared to no screening) and incremental cost-effectiveness ratios (ICERs). A willingness-to-pay threshold of $100 000 per life-years gained (LYG) was used to determine the optimal screening strategy.
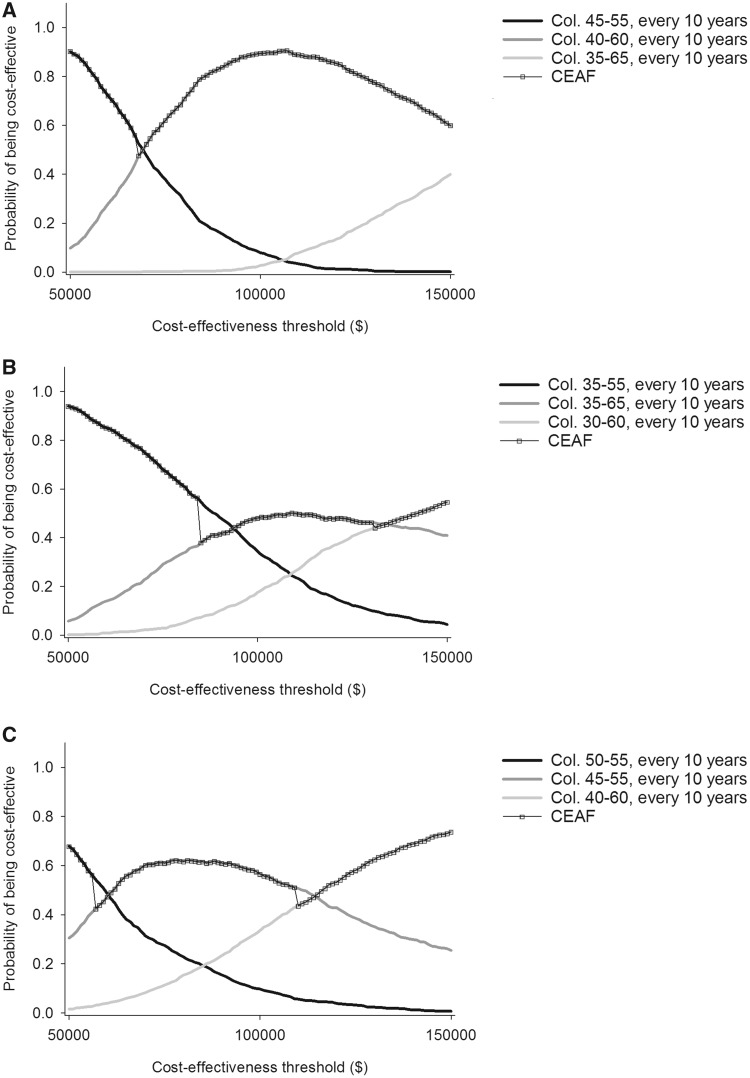
Results: Compared to no screening, the US Preventive Services Task Force's average risk screening schedule prevented up to 73.2% of CRC deaths in CCS. The optimal strategy of screening every 10 years from age 40 to 60 years averted 79.2% of deaths, with ICER of $67 000/LYG. Among CCS treated with APRT, colonoscopy every 10 years from age 35 to 65 years was optimal (CRC deaths averted: 82.3%; ICER: $92 000/LYG), whereas among those not previously treated with APRT, screening from age 45 to 55 years every 10 years was optimal (CRC deaths averted: 72.7%; ICER: $57 000/LYG).
Conclusions: Early initiation of colonoscopy screening for CCS is cost-effective, especially among those treated with APRT.
© The Author(s) 2019. Published by Oxford University Press.
Figures
Comment in
-
Colorectal Cancer Screening in Childhood Cancer Survivors.J Natl Cancer Inst. 2019 Nov 1;111(11):1114-1115. doi: 10.1093/jnci/djz063. J Natl Cancer Inst. 2019. PMID: 30980664 Free PMC article. No abstract available.
References
-
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Limited Use, Nov 2002 Sub (1973–2000). National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch. Released April 2003, based on the November 2002 submission.
-
- Mertens AC, Yasui Y, Neglia JP, et al. Late mortality experience in five-year survivors of childhood and adolescent cancer: the Childhood Cancer Survivor Study. J Clin Oncol. 2001;1913:3163–3172. - PubMed
-
- Daly PE, Samiee S, Cino M, et al. High prevalence of adenomatous colorectal polyps in young cancer survivors treated with abdominal radiation therapy: results of a prospective trial. Gut. 2017;6610:1797–1801. - PubMed
-
- Nottage K, McFarlane J, Krasin MJ, et al. Secondary colorectal carcinoma after childhood cancer. J Clin Oncol. 2012;3020:2552–2558. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
