

Acute withdrawal and botulinum toxin A in chronic migraine with medication overuse: a double-blind randomized controlled trial
- PMID: 30982843
- PMCID: PMC6511115
- DOI: 10.1093/brain/awz052
Acute withdrawal and botulinum toxin A in chronic migraine with medication overuse: a double-blind randomized controlled trial
Abstract
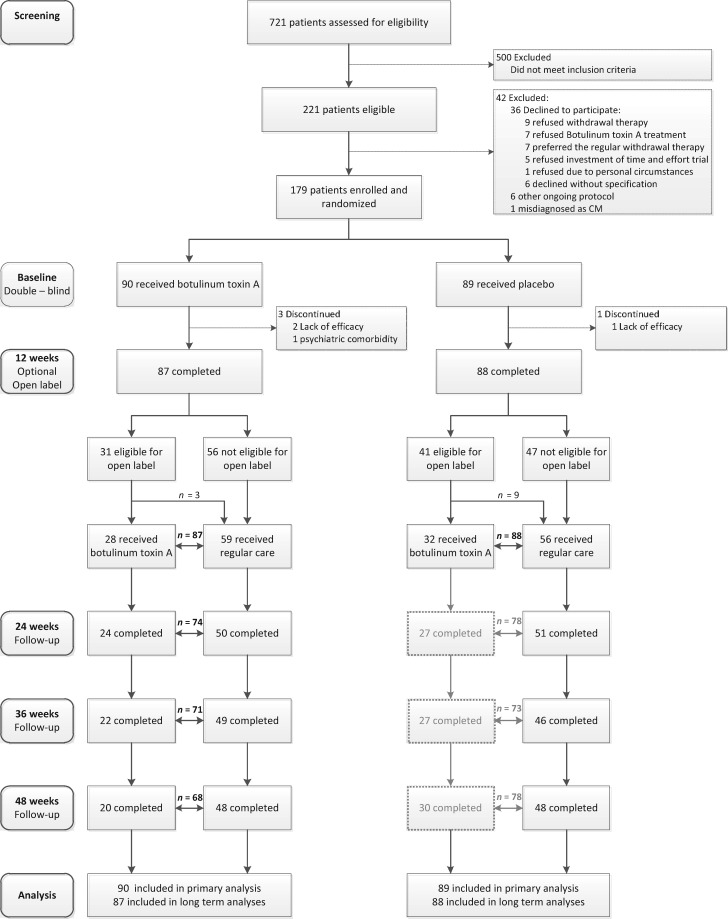
Botulinum toxin A (BTA) is widely used as treatment of chronic migraine. Efficacy in studies, however, was only modest and likely influenced by unblinding due to BTA-induced removal of forehead wrinkles. Moreover, most study participants were overusing acute headache medications and might have benefitted from withdrawal. We assessed in a double blind, placebo-controlled, randomized clinical trial whether add-on therapy with BTA enhances efficacy of acute withdrawal. Participants were enrolled between December 2012 and February 2015, with follow-up to January 2016, in a single academic hospital in the Netherlands. A total of 179 participants, male and female, aged 18-65, diagnosed with chronic migraine and overuse of acute headache medication were included. All participants were instructed to withdraw acutely from all medication for a 12-week period, in an outpatient setting. In addition, they were randomly assigned (1:1) to 31 injections with BTA (155 units) or placebo (saline); to prevent unblinding, placebo-treated participants received low doses of BTA (17.5 units in total) in the forehead, along with saline injections outside the forehead region. Primary endpoint was percentage change in monthly headache days from baseline to the last 4 weeks of double-blind treatment (Weeks 9-12). Among 179 randomized patients, 90 received BTA and 89 received placebo, and 175 (98%) completed the double-blind phase. All 179 patients were included in the intention-to-treat analyses. BTA did not reduce monthly headache days versus placebo (-26.9% versus -20.5%; difference -6.4%; 95% confidence interval: -15.2 to 2.4; P = 0.15). Absolute changes in migraine days at 12 weeks for BTA versus placebo were -6.2 versus -7.0 (difference: 0.8; 95% confidence interval: -1.0 to 2.7; P = 0.38). Other secondary endpoints, including measures for disability and quality of life, did also not differ. Withdrawal was well tolerated and blinding was successful. Thus, in patients with chronic migraine and medication overuse, BTA does not afford any additional benefit over acute withdrawal alone. Acute withdrawal should be tried first before initiating more expensive treatment with BTA.
Keywords: botulinum toxin A; chronic migraine; detoxification; medication overuse; withdrawal.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures



Comment in
-
OnabotulinumtoxinA should be considered in medication overuse withdrawal in patients with chronic migraine.Brain. 2020 Jan 1;143(1):e5. doi: 10.1093/brain/awz366. Brain. 2020. PMID: 31782764 No abstract available.
-
Reply: OnabotulinumtoxinA should be considered in medication overuse withdrawal in patients with chronic migraine.Brain. 2020 Jan 1;143(1):e6. doi: 10.1093/brain/awz368. Brain. 2020. PMID: 31782777 Free PMC article. No abstract available.
References
-
- Aurora SK, Dodick DW, Turkel CC, DeGryse RE, Silberstein SD, Lipton RB et al. . OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010; 30: 804–14. - PubMed
-
- Australian Government. Australian Public Assessment Report for Botulinum Toxin Type A Proprietary Product Name: Botox [Internet]. 2011. https://www.tga.gov.au/sites/default/files/auspar-botox.pdf (11 July 2017, date last accessed).
-
- Bigal ME, Edvinsson L, Rapoport AM, Lipton RB, Spierings ELH, Diener HC et al. . Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of chronic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol 2015a; 14: 1091–100. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
