

Serum Zinc-α2-Glycoprotein Levels Were Decreased in Patients With Premature Coronary Artery Disease
- PMID: 30984114
- PMCID: PMC6449697
- DOI: 10.3389/fendo.2019.00197
Serum Zinc-α2-Glycoprotein Levels Were Decreased in Patients With Premature Coronary Artery Disease
Abstract
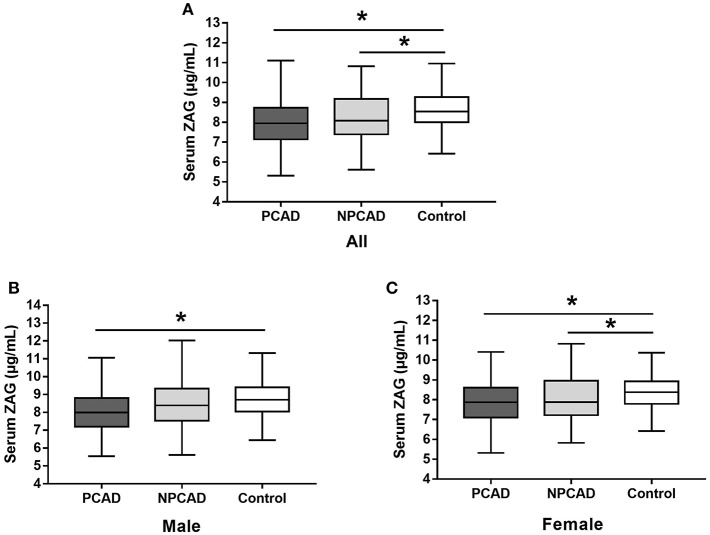
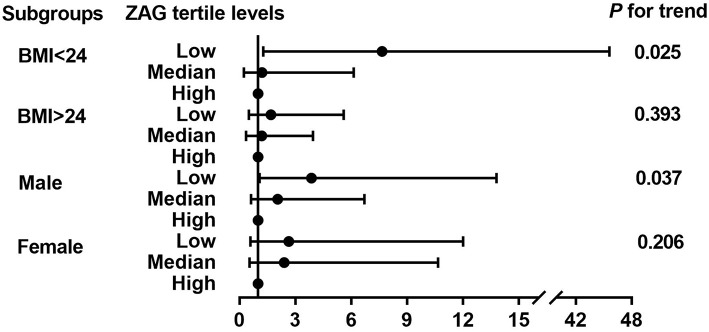
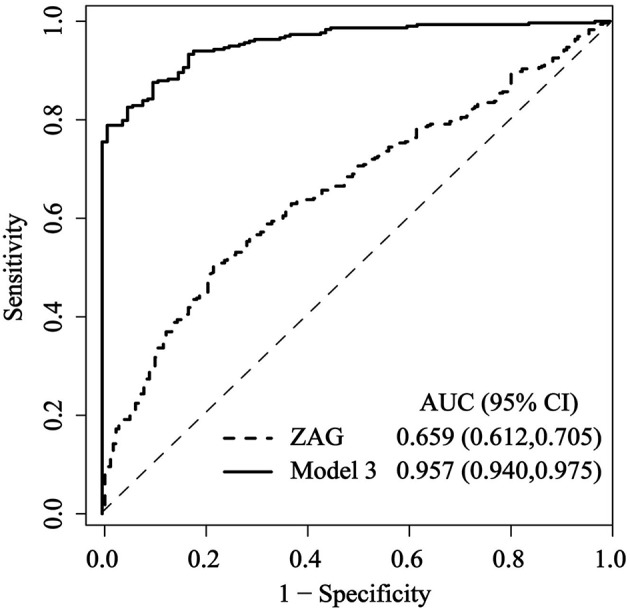
Objectives: To explore serum zinc-α2-glycoprotein (ZAG) changes in patients with or without premature coronary artery disease (PCAD) and its association with several cardiovascular risk factors. Methods: A total of 3,364 patients who were undergone coronary angiography in Peking Union Medical College Hospital were screened. According to the degree of coronary artery stenosis, the number of 364 patients with PCAD (age <55 years in males and <65 years in females) and 126 age and gender matched patients without premature coronary artery disease (NPCAD) were recruited in our present study. In addition, 182 age and gender matched healthy controls were also enrolled. Serum ZAG levels were determined by enzyme-linked immunosorbent assay (ELISA) method. Results: Serum ZAG were significantly lower in the PCAD (8.03 ± 1.01 vs. 8.78 ± 1.89 μg/mL, p < 0.05) and NPCAD groups (8.28 ± 1.61 vs. 8.78 ± 1.89 μg/mL, p < 0.05), respectively, when compared with the controls. Multiple regression analysis showed that PCAD was independently associated with serum ZAG levels (B = -0.289, p = 0.002). The probability of PCAD in subjects with low tertile ZAG levels was 2.48-fold higher than those with high tertile levels after adjusting for other confounders [OR = 3.476, 95% CI 1.387-8.711, p = 0.008]. This phenomenon was more likely to be observed in male subjects with BMI <24 kg/m2. The receiver operating curve (ROC) analysis showed a weak diagnostic performance of serum ZAG for PCAD (AUC = 0.659, 95% CI 0.612-0.705, p < 0.05). At the cutoff value of 7.955 μg/mL serum ZAG, the sensitivity and specificity for differentiating patients with PCAD from controls were 50.5 and 78.0%, respectively. The combination of ZAG with other clinical variables including age, gender, BMI, SBP, FBG, TC, HDL-C, Cr, and Urea had significantly improved the diagnosis accuracy with a sensitivity of 82.6%, a specificity of 95.0%, and AUC of 0.957 (95% CI, 0.940-0.975, p < 0.05). Conclusion: Serum ZAG levels were firstly found to be decreased in Chinese PCAD patients. Subjects with lower ZAG levels were more likely to have PCAD, especially for male subjects with BMI <24 kg/m2. ZAG might be the potential diagnostic biomarkers for PCAD patients, and the combination of ZAG and clinical variables had higher discriminative performance.
Keywords: body mass index (BMI); diagnostic biomarker; non-premature coronary artery disease (NPCAD); premature coronary artery disease (PCAD); zinc-α2-glycoprotein (ZAG).
Figures
Similar articles
-
High serum clusterin levels are associated with premature coronary artery disease in a Chinese population.Diabetes Metab Res Rev. 2019 May;35(4):e3128. doi: 10.1002/dmrr.3128. Epub 2019 Feb 7. Diabetes Metab Res Rev. 2019. PMID: 30659732
-
Serum Zinc-α2-Glycoprotein Levels in Patients with or without Coronary Artery Disease in Chinese North Population.Int J Endocrinol. 2020 Feb 27;2020:7864721. doi: 10.1155/2020/7864721. eCollection 2020. Int J Endocrinol. 2020. PMID: 32184822 Free PMC article.
-
Identification of U-shaped curve relation between proneurotensin and risk of coronary artery disease (CAD) in patients with premature CAD.Nutr Metab Cardiovasc Dis. 2020 Mar 9;30(3):483-491. doi: 10.1016/j.numecd.2019.10.009. Epub 2019 Oct 24. Nutr Metab Cardiovasc Dis. 2020. PMID: 31926821
-
Premature Coronary Artery Disease and Plasma Levels of Interleukins; a Systematic Scoping Review and Meta-Analysis.Arch Acad Emerg Med. 2022 Jun 27;10(1):e51. doi: 10.22037/aaem.v10i1.1605. eCollection 2022. Arch Acad Emerg Med. 2022. PMID: 36033992 Free PMC article.
-
What Causes Premature Coronary Artery Disease?Curr Atheroscler Rep. 2024 Jun;26(6):189-203. doi: 10.1007/s11883-024-01200-y. Epub 2024 Apr 4. Curr Atheroscler Rep. 2024. PMID: 38573470 Review.
Cited by
-
Changes in AZGP1 Serum Levels and Correlation With Pulse Wave Velocity After Kidney Transplantation.Front Cardiovasc Med. 2021 Jul 5;8:692213. doi: 10.3389/fcvm.2021.692213. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34291094 Free PMC article.
-
Development of a prediction model for mortality and cardiovascular outcomes in older adults taking into account AZGP1.Sci Rep. 2021 Jun 3;11(1):11792. doi: 10.1038/s41598-021-91169-4. Sci Rep. 2021. PMID: 34083628 Free PMC article.
-
Association between dietary zinc intake and olfactory dysfunction: a study based on the NHANES database.Eur Arch Otorhinolaryngol. 2024 May;281(5):2441-2450. doi: 10.1007/s00405-023-08427-6. Epub 2024 Jan 5. Eur Arch Otorhinolaryngol. 2024. PMID: 38180607
-
Relationship between Copper, Zinc, and Copper-to-Zinc Ratio in Hair and Severity of Coronary Artery Disease according to the SYNTAX Score.Biology (Basel). 2023 Nov 7;12(11):1407. doi: 10.3390/biology12111407. Biology (Basel). 2023. PMID: 37998006 Free PMC article.
-
Adipose and serum zinc alpha-2-glycoprotein (ZAG) expressions predict longitudinal change of adiposity, wasting and predict survival in dialysis patients.Sci Rep. 2022 May 31;12(1):9087. doi: 10.1038/s41598-022-13149-6. Sci Rep. 2022. PMID: 35641588 Free PMC article.
References
-
- Separham HSK. The relative impact of smoking or Hypertension on severity of premature coronary artery disease. Iran Red Crescent Me. (2007) 4:177–8.
LinkOut - more resources
Full Text Sources
Miscellaneous