

Therapeutic Potential of Regulatory T Cells in Preeclampsia-Opportunities and Challenges
- PMID: 30984163
- PMCID: PMC6448013
- DOI: 10.3389/fimmu.2019.00478
Therapeutic Potential of Regulatory T Cells in Preeclampsia-Opportunities and Challenges
Abstract
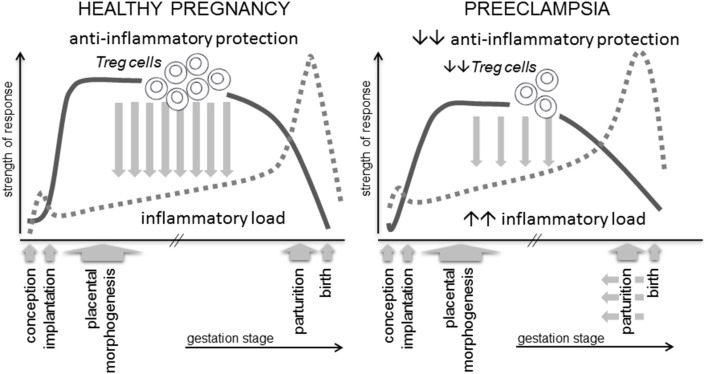
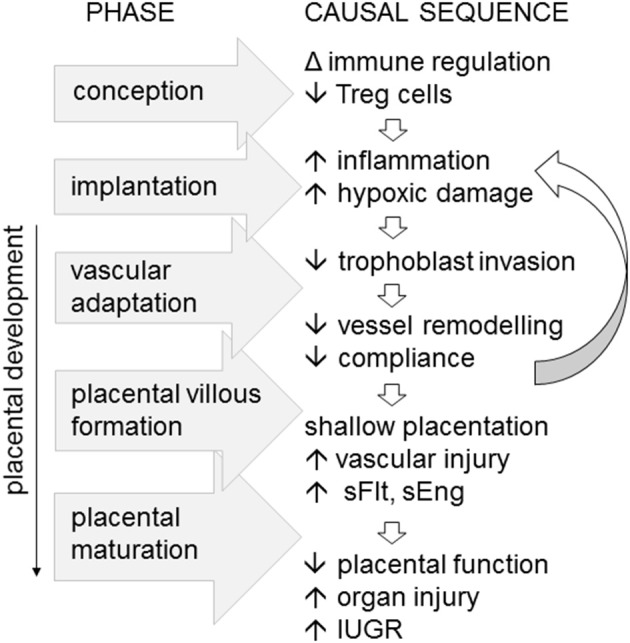
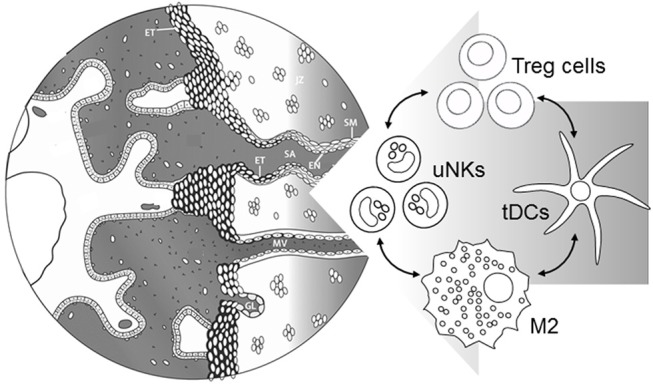
Inflammation is a central feature and is implicated as a causal factor in preeclampsia and other hypertensive disorders of pregnancy. Inflammatory mediators and leukocytes, which are elevated in peripheral blood and gestational tissues, contribute to the uterine vascular anomalies and compromised placental function that characterize particularly the severe, early onset form of disease. Regulatory T (Treg) cells are central mediators of pregnancy tolerance and direct other immune cells to counteract inflammation and promote robust placentation. Treg cells are commonly perturbed in preeclampsia, and there is evidence Treg cell insufficiency predates onset of symptoms. A causal role is implied by mouse studies showing sufficient numbers of functionally competent Treg cells must be present in the uterus from conception, to support maternal vascular adaptation and prevent later placental inflammatory pathology. Treg cells may therefore provide a tractable target for both preventative strategies and treatment interventions in preeclampsia. Steps to boost Treg cell activity require investigation and could be incorporated into pregnancy planning and preconception care. Pharmacological interventions developed to target Treg cells in autoimmune conditions warrant consideration for evaluation, utilizing rigorous clinical trial methodology, and ensuring safety is paramount. Emerging cell therapy tools involving in vitro Treg cell generation and/or expansion may in time become relevant. The success of preventative and therapeutic approaches will depend on resolving several challenges including developing informative diagnostic tests for Treg cell activity applicable before conception or during early pregnancy, selection of relevant patient subgroups, and identification of appropriate windows of gestation for intervention.
Keywords: Treg cells; embryo implantation; immune tolerance; inflammation; maternal vascular adaptation; placenta; preeclampsia; pregnancy.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources