

Local and Distant Recurrence in Resected Sacral Chordomas: A Systematic Review and Pooled Cohort Analysis
- PMID: 30984500
- PMCID: PMC6448196
- DOI: 10.1177/2192568217741114
Local and Distant Recurrence in Resected Sacral Chordomas: A Systematic Review and Pooled Cohort Analysis
Abstract
Study design: Systematic review.
Objectives: Sacral chordomas are rare, primary tumors of the spine, best treated with en bloc resection. The purpose of this study was to assess the literature for resected sacral chordoma and to quantify the prevalence of, risk factors for, and treatment outcomes of local and distant recurrence therein.
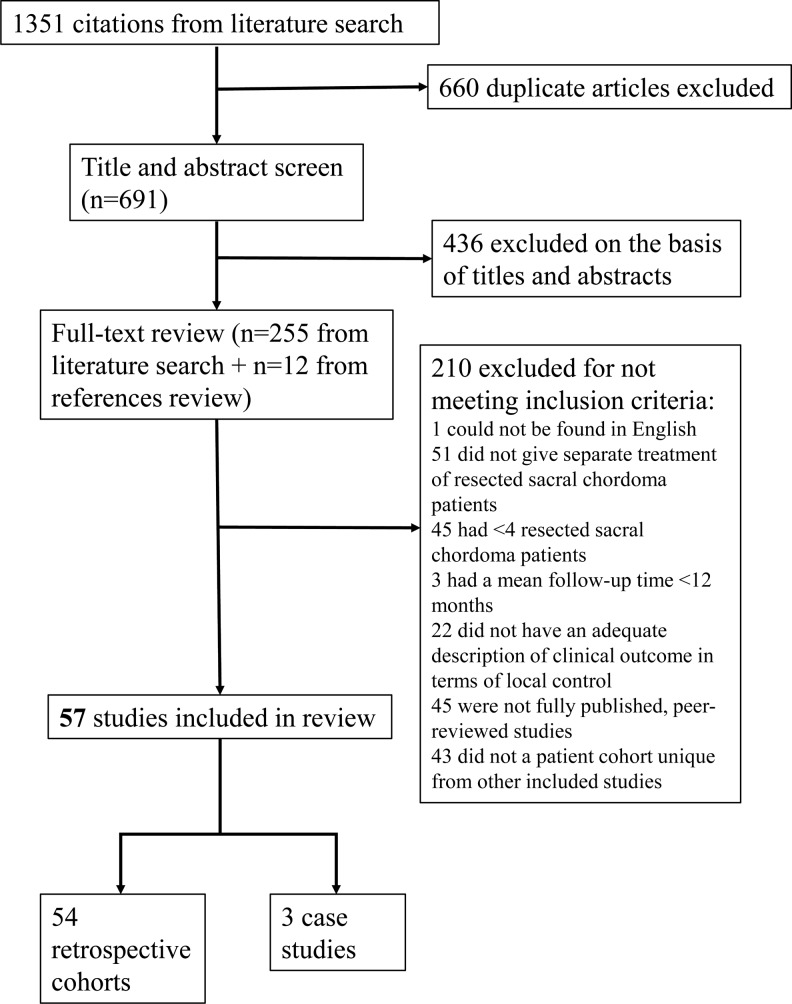
Methods: We searched 5 online databases from January 1980 to May 2016 to find articles that report survival, recurrence outcomes, and/or prognostic factors for the resected sacral chordoma patient population. Characteristics and clinical outcomes of the pooled cohort are reported. Fisher exact tests, unpaired t tests, and one-way analysis of variance were used to investigate patient- and treatment-associated prognostic factors for local and distant recurrence. Survival analyses were performed for time to local recurrence and death. The protocol's PROSPERO ID is CRD42015024384.
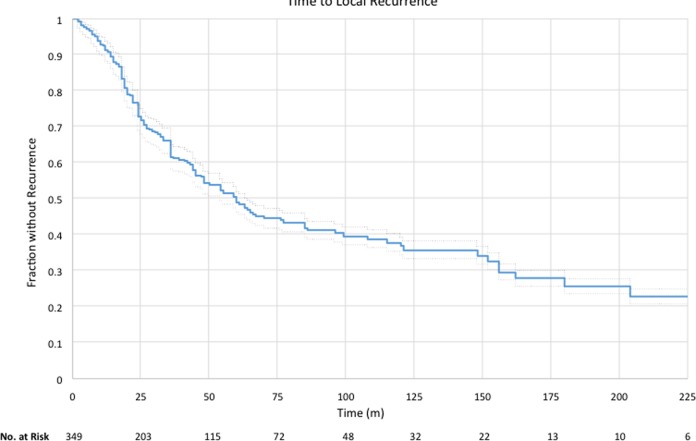
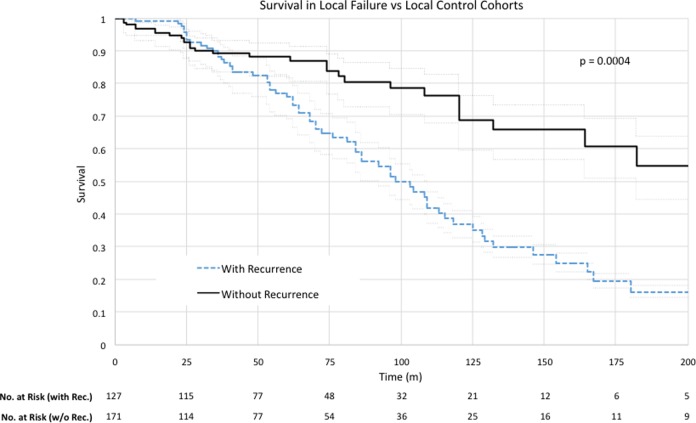
Results: Fifty-seven studies, with 1235 unique sacral chordoma patients, were included in this review. Local and distant recurrence occurred in 42.6% and 22.4% of patients with adequate follow-up, respectively. Kaplan-Meier overall median survival for patients with and without recurrence were 98 and 209 months after surgery, respectively. Wide surgical margin was associated with a lower rate of local recurrence; and wide surgical margin, female sex, and patient age ≥65 years were associated with lower rates of distant recurrence.
Conclusions: While surgical margin remains the most significant prognostic factor for local and distant recurrence, combined surgical approach may be associated with local recurrence. Male sex and age <65 years may be associated with distant recurrence. Patients with risk factors for recurrence should undergo close monitoring to maximize survival.
Keywords: lumbosacral; recurrent chordoma; sacral chordoma; sacrum; systematic review; tumors.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Rory Goodwin: UNCF Merck Postdoctoral Fellow and has received an award from the Burroughs Wellcome Fund. Daniel Kerekes: None. A. Karim Ahmed: Has received an award from the NREF Medical Student Summer Research Fellowship. Jorrit-Jan Verlaan: None. Chetan Bettegowda: None. Nancy Abu-Bonsrah: None. Daniel M. Sciubba: Consultant for Medtronic, Globus, DePuy, Styrker, and Orthofix.
Figures
References
-
- Gulluoglu S, Turksoy O, Kuskucu A, Ture U, Bayrak OF. The molecular aspects of chordoma. Neurosurg Rev. 2016;39:185–196. - PubMed
-
- McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM. Chordoma: incidence and survival patterns in the United States, 1973-1995. Cancer Causes Control. 2001;12:1–11. - PubMed
-
- Sciubba DM, Cheng JJ, Petteys RJ, Weber KL, Frassica DA, Gokaslan ZL. Chordoma of the sacrum and vertebral bodies. J Am Acad Orthop Surg. 2009;17:708–717. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
