

Left Ventricular Longitudinal Contractility Predicts Acute-on-Chronic Liver Failure Development and Mortality After Transjugular Intrahepatic Portosystemic Shunt
- PMID: 30984902
- PMCID: PMC6444053
- DOI: 10.1002/hep4.1308
Left Ventricular Longitudinal Contractility Predicts Acute-on-Chronic Liver Failure Development and Mortality After Transjugular Intrahepatic Portosystemic Shunt
Abstract
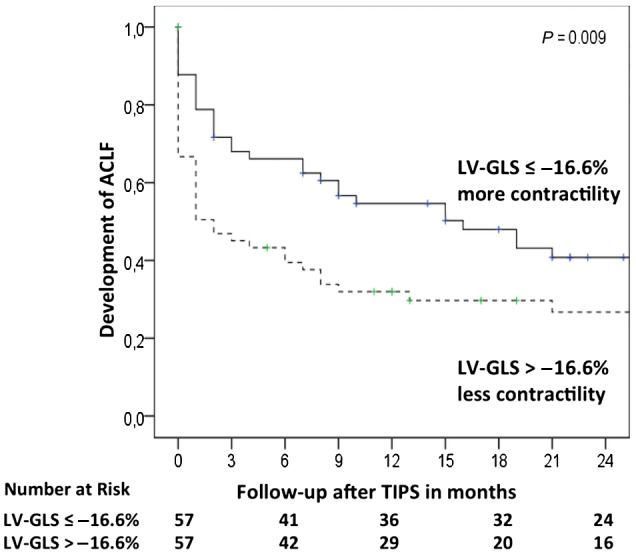
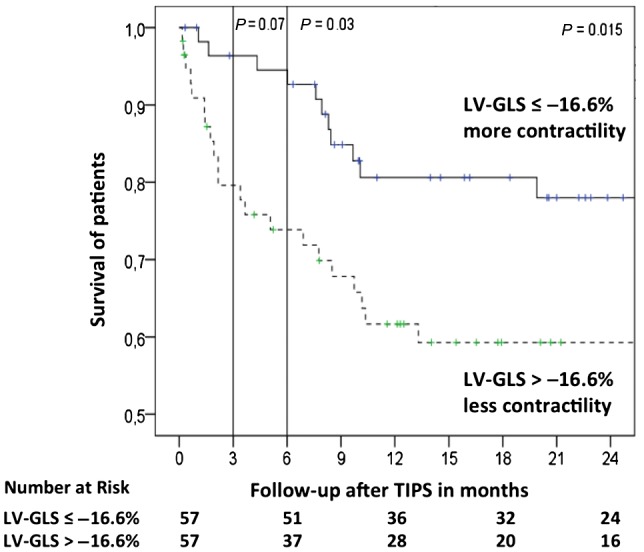
Acute deterioration of liver cirrhosis (e.g., infections, acute-on-chronic liver failure [ACLF]) requires an increase in cardiac contractility. The insufficiency to respond to these situations could be deleterious. Left ventricular global longitudinal strain (LV-GLS) has been shown to reflect left cardiac contractility in cirrhosis better than other parameters and might bear prognostic value. Therefore, this retrospective study investigated the role of LV-GLS in the outcome after transjugular intrahepatic portosystemic shunt (TIPS) and the development of ACLF. We included 114 patients (48 female patients) from the Noninvasive Evaluation Program for TIPS and Their Follow-Up Network (NEPTUN) cohort. This number provided sufficient quality and structured follow-up with the possibility of calculating major scores (Child, Model for End-Stage Liver Disease [MELD], Chronic Liver Failure Consortium acute decompensation [CLIF-C AD] scores) and recording of the events (development of decompensation episode and ACLF). We analyzed the association of LV-GLS with overall mortality and development of ACLF in patients with TIPS. LV-GLS was independently associated with overall mortality (hazard ratio [HR], 1.123; 95% confidence interval [CI],1.010-1.250) together with aspartate aminotransferase (HR, 1.009; 95% CI, 1.004-1.014) and CLIF-C AD score (HR, 1.080; 95% CI, 1.018-1.137). Area under the receiver operating characteristic curve (AUROC) analysis for LV-GLS for overall survival showed higher area under the curve (AUC) than MELD and CLIF-C AD scores (AUC, 0.688 versus 0.646 and 0.573, respectively). The best AUROC-determined LV-GLS cutoff was -16.6% to identify patients with a significantly worse outcome after TIPS at 3 months, 6 months, and overall. LV-GLS was independently associated with development of ACLF (HR, 1.613; 95% CI, 1.025-2.540) together with a MELD score above 15 (HR, 2.222; 95% CI, 1.400-3.528). Conclusion: LV-GLS is useful for identifying patients at risk of developing ACLF and a worse outcome after TIPS. Although validation is required, this tool might help to stratify risk in patients receiving TIPS.
Figures
Similar articles
-
Preoperative TIPS prevents the development of postoperative acute-on-chronic liver failure in patients with high CLIF-C AD score.JHEP Rep. 2022 Jan 21;4(3):100442. doi: 10.1016/j.jhepr.2022.100442. eCollection 2022 Mar. JHEP Rep. 2022. PMID: 35198929 Free PMC article.
-
Chronic liver failure-consortium acute-on-chronic liver failure and acute decompensation scores predict mortality in Brazilian cirrhotic patients.World J Gastroenterol. 2017 Jul 28;23(28):5237-5245. doi: 10.3748/wjg.v23.i28.5237. World J Gastroenterol. 2017. PMID: 28811718 Free PMC article.
-
CLIF-C AD score predicts survival benefit from pre-emptive TIPS in individuals with Child-Pugh B cirrhosis and acute variceal bleeding.JHEP Rep. 2022 Oct 28;4(12):100621. doi: 10.1016/j.jhepr.2022.100621. eCollection 2022 Dec. JHEP Rep. 2022. PMID: 36439638 Free PMC article.
-
Sarcopenia Is Associated With Development of Acute-on-Chronic Liver Failure in Decompensated Liver Cirrhosis Receiving Transjugular Intrahepatic Portosystemic Shunt.Clin Transl Gastroenterol. 2019 Apr;10(4):e00025. doi: 10.14309/ctg.0000000000000025. Clin Transl Gastroenterol. 2019. PMID: 30939488 Free PMC article.
-
Elective Surgery but not Transjugular Intrahepatic Portosystemic Shunt Precipitates Acute-On-Chronic Liver Failure.Hepatol Commun. 2021 Mar 26;5(7):1265-1277. doi: 10.1002/hep4.1712. eCollection 2021 Jul. Hepatol Commun. 2021. PMID: 34278174 Free PMC article.
Cited by
-
Utilizing the gut microbiome in decompensated cirrhosis and acute-on-chronic liver failure.Nat Rev Gastroenterol Hepatol. 2021 Mar;18(3):167-180. doi: 10.1038/s41575-020-00376-3. Epub 2020 Nov 30. Nat Rev Gastroenterol Hepatol. 2021. PMID: 33257833 Review.
-
Cardiac Remodeling and Arrhythmic Burden in Pre-Transplant Cirrhotic Patients: Pathophysiological Mechanisms and Management Strategies.Biomedicines. 2025 Mar 28;13(4):812. doi: 10.3390/biomedicines13040812. Biomedicines. 2025. PMID: 40299454 Free PMC article. Review.
-
Transjugular intrahepatic portosystemic stent-shunt in the management of portal hypertension.Gut. 2020 Jul;69(7):1173-1192. doi: 10.1136/gutjnl-2019-320221. Epub 2020 Feb 29. Gut. 2020. PMID: 32114503 Free PMC article.
-
Transjugular intrahepatic portosystemic shunt in cirrhosis: An exhaustive critical update.World J Gastroenterol. 2020 Oct 7;26(37):5561-5596. doi: 10.3748/wjg.v26.i37.5561. World J Gastroenterol. 2020. PMID: 33088154 Free PMC article. Review.
-
Unveiling the impact of cirrhotic cardiomyopathy on portal hemodynamics and survival after transjugular intrahepatic portosystemic shunt: a prospective study.Abdom Radiol (NY). 2024 Oct;49(10):3507-3516. doi: 10.1007/s00261-024-04446-x. Epub 2024 Jun 20. Abdom Radiol (NY). 2024. PMID: 38900326
References
-
- Trebicka J. Predisposing factors in acute‐on‐chronic liver failure. Semin Liver Dis 2016;36:167‐173. - PubMed
-
- Trebicka J. Emergency TIPS in a Child‐Pugh B patient: when does the window of opportunity open and close? J Hepatol 2017;66:442‐450. - PubMed
-
- Trebicka J. Does transjugular intrahepatic portosystemic shunt stent differentially improve survival in a subset of cirrhotic patients? Semin Liver Dis 2018;38:87‐96. - PubMed
-
- Busk TM, Bendtsen F, Poulsen JH, Clemmesen JO, Larsen FS, Goetze JP, et al. Transjugular intrahepatic portosystemic shunt: impact on systemic hemodynamics and renal and cardiac function in patients with cirrhosis. Am J Physiol Gastrointest Liver Physiol 2018;314:G275‐G286. - PubMed
-
- Merli M, Valeriano V, Funaro S, Attili AF, Masini A, Efrati C, et al. Modifications of cardiac function in cirrhotic patients treated with transjugular intrahepatic portosystemic shunt (TIPS). Am J Gastroenterol 2002;97:142‐148. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
