

Three-dimensional reconstruction of defects in congenital diaphragmatic hernia: a fetal MRI study
- PMID: 30985045
- PMCID: PMC6619026
- DOI: 10.1002/uog.20296
Three-dimensional reconstruction of defects in congenital diaphragmatic hernia: a fetal MRI study
Abstract
Objective: To assess the clinical feasibility and validity of fetal magnetic resonance imaging (MRI)-based three-dimensional (3D) reconstruction to locate, classify and quantify diaphragmatic defects in congenital diaphragmatic hernia (CDH).
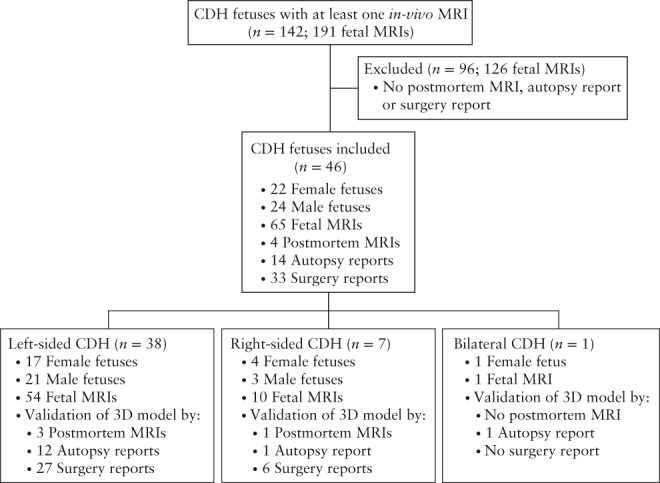
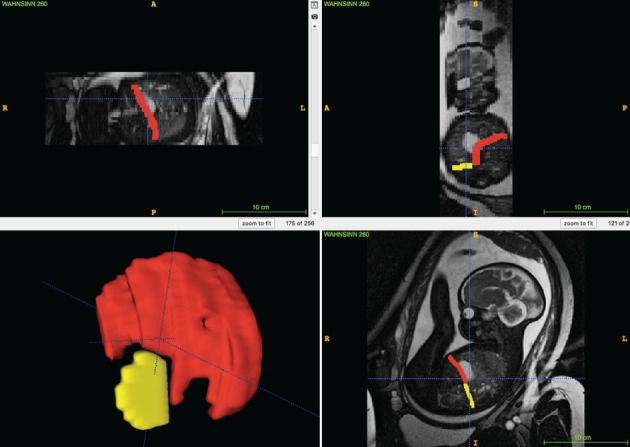
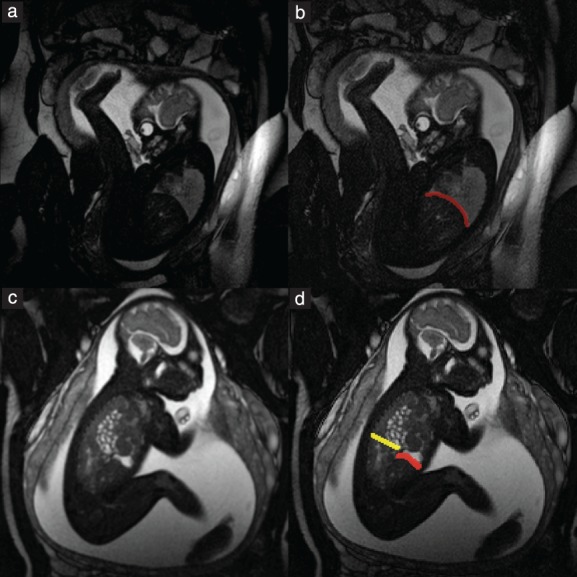
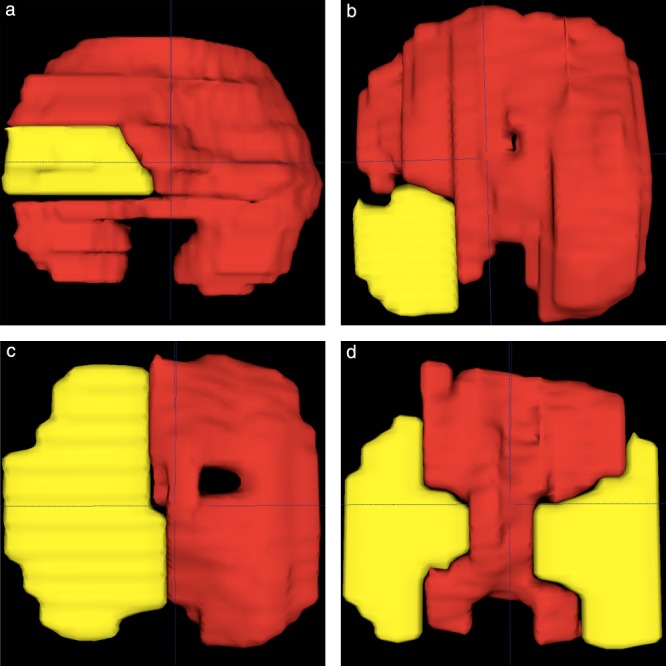
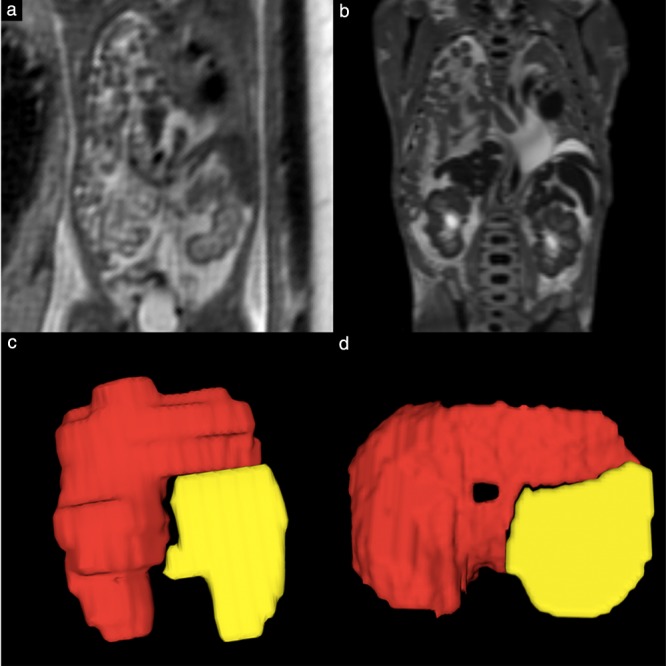
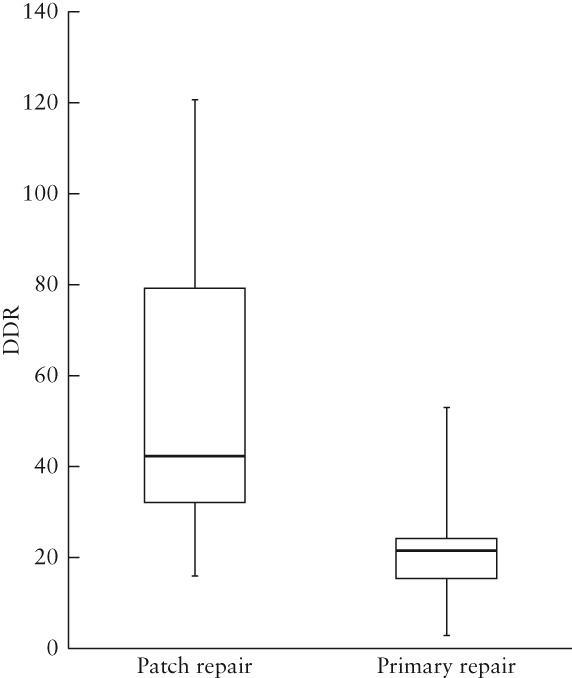
Methods: This retrospective study included 46 cases of CDH which underwent a total of 69 fetal MRI scans (65 in-vivo and four postmortem) at the Medical University of Vienna during the period 1 January 2002 to 1 January 2017. Scans were performed between 16 and 38 gestational weeks using steady-state free precession, T2-weighted and T1-weighted sequences. MRI data were retrieved from the hospital database and manual segmentation of the diaphragm was performed with the open-source software, ITK-SNAP. The resulting 3D models of the fetal diaphragm and its defect(s) were validated by postmortem MRI segmentation and/or comparison of 3D model-based classification of the defect with a reference classification based on autopsy and/or surgery reports. Surface areas of the intact diaphragm and of the defect were measured and used to calculate defect-diaphragmatic ratios (DDR). The need for prosthetic patch repair and, in cases with repeated in-vivo fetal MRI scans, diaphragm growth dynamics, were analyzed based on DDR.
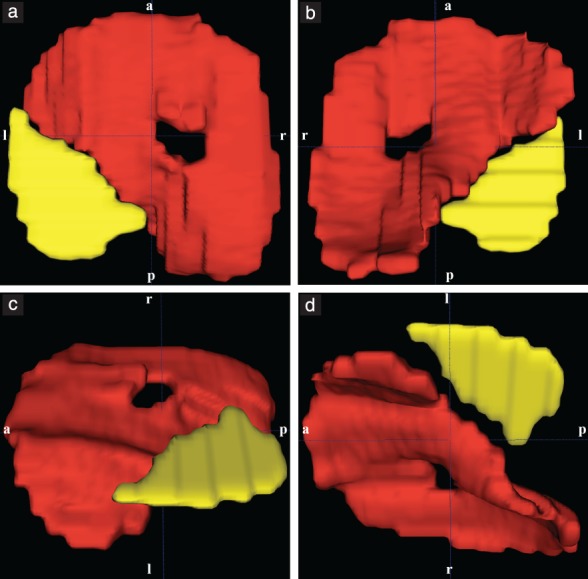
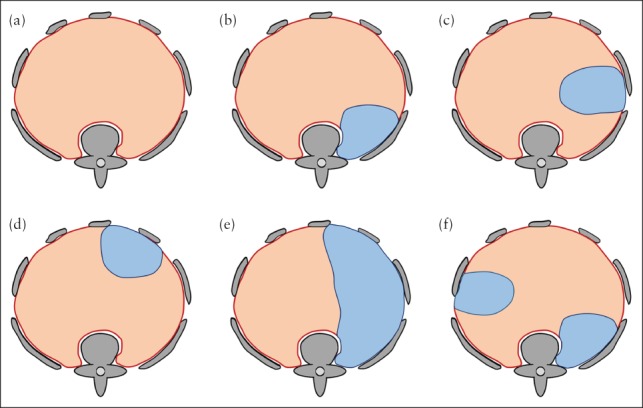
Results: Fetal MRI-based manual segmentation of the diaphragm in CDH was feasible for all 65 (100%) of the in-vivo fetal MRI scans. Based on the 3D diaphragmatic models, one bilateral and 45 unilateral defects (n = 47) were further classified as posterolateral (23/47, 48.9%), lateral (7/47, 14.9%) or hemidiaphragmatic (17/47, 36.2%) defects, and none (0%) was classified as anterolateral. This classification of defect location was correct in all 37 (100%) of the cases in which this information could be verified. Nineteen cases had a follow-up fetal MRI scan; in five (26.3%) of these, the initial CDH classification was altered by the results of the second scan. Thirty-three fetuses underwent postnatal diaphragmatic surgical repair; 20 fetuses (all of those with DDR ≥ 54 and 88% of those with DDR > 30) received a diaphragmatic patch, while the other 13 underwent primary surgical repair. Individual DDRs at initial and at follow-up in-vivo fetal MRI correlated significantly (P < 0.001).
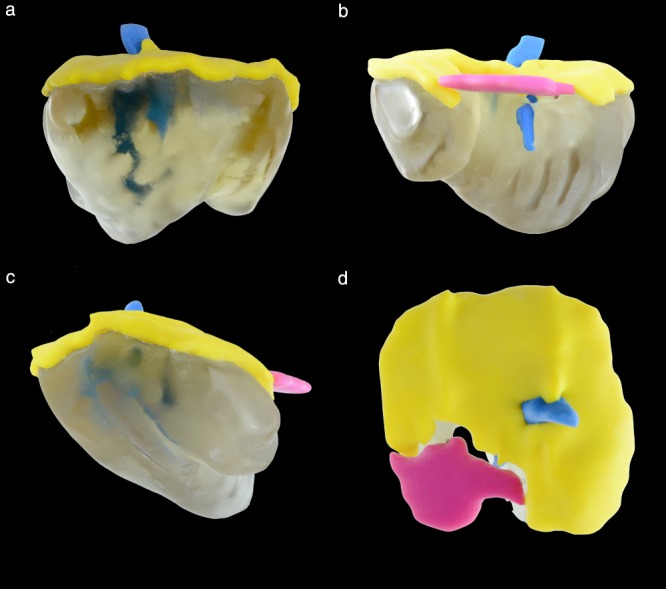
Conclusions: MRI-based 3D reconstruction of the fetal diaphragm in CDH has been validated to visualize, locate, classify and quantify the defect. Planning of postnatal surgery may be optimized by MRI-based prediction of the necessity for patch placement and the ability to personalize patch design based on 3D-printable templates. Copyright © 2019 ISUOG. Published by John Wiley & Sons Ltd.
Keywords: CDH; CDH classification; CDH typology; MRI; MRI-based segmentation; congenital diaphragmatic hernia; fetal MRI; fetal diaphragm.
Copyright © 2019 ISUOG. Published by John Wiley & Sons Ltd.
Figures
References
-
- McGivern MR, Best KE, Rankin J, Wellesley D, Greenlees R, Addor MC, Arriola L, de Walle H, Barisic I, Beres J, Bianchi F, Calzolari E, Doray B, Draper ES, Garne E, Gatt M, Haeusler M, Khoshnood B, Klungsoyr K, Latos‐Bielenska A, O'Mahony M, Braz P, McDonnell B, Mullaney C, Nelen V, Queisser‐Luft A, Randrianaivo H, Rissmann A, Rounding C, Sipek A, Thompson R, Tucker D, Wertelecki W, Martos C. Epidemiology of congenital diaphragmatic hernia in Europe: a register‐based study. Arch Dis Child Fetal Neonatal Ed 2015; 100: F137–144. - PubMed
-
- Balayla J, Abenhaim HA. Incidence, predictors and outcomes of congenital diaphragmatic hernia: a population‐based study of 32 million births in the United States. J Matern Fetal Neonatal Med 2014; 27: 1438–1444. - PubMed
-
- Langham MR, Jr , Kays DW, Ledbetter DJ, Frentzen B, Sanford LL, Richards DS. Congenital diaphragmatic hernia. Epidemiology and outcome. Clin Perinatol 1996; 23: 671–688. - PubMed
-
- Kitagawa M, Hislop A, Boyden EA, Reid L. Lung hypoplasia in congenital diaphragmatic hernia. A quantitative study of airway, artery, and alveolar development. Br J Surg 1971; 58: 342–346. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical