

Staged Implementation of Awakening and Breathing, Coordination, Delirium Monitoring and Management, and Early Mobilization Bundle Improves Patient Outcomes and Reduces Hospital Costs
- PMID: 30985390
- PMCID: PMC6579661
- DOI: 10.1097/CCM.0000000000003765
Staged Implementation of Awakening and Breathing, Coordination, Delirium Monitoring and Management, and Early Mobilization Bundle Improves Patient Outcomes and Reduces Hospital Costs
Abstract
Objectives: To measure the impact of staged implementation of full versus partial ABCDE bundle on mechanical ventilation duration, ICU and hospital lengths of stay, and cost.
Design: Prospective cohort study.
Setting: Two medical ICUs within Montefiore Healthcare Center (Bronx, NY).
Patients: One thousand eight hundred fifty-five mechanically ventilated patients admitted to ICUs between July 2011 and July 2014.
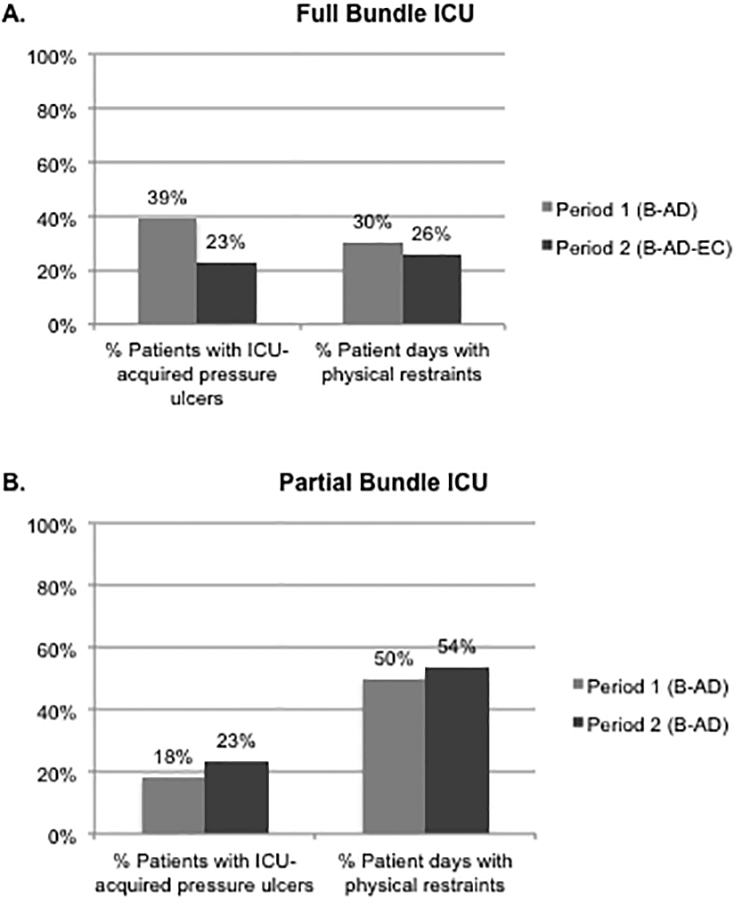
Interventions: At baseline, spontaneous (B)reathing trials (B) were ongoing in both ICUs; in period 1, (A)wakening and (D)elirium (AD) were implemented in both full and partial bundle ICUs; in period 2, (E)arly mobilization and structured bundle (C)oordination (EC) were implemented in the full bundle (B-AD-EC) but not the partial bundle ICU (B-AD).
Measurements and main results: In the full bundle ICU, 95% patient days were spent in bed before EC (period 1). After EC was implemented (period 2), 65% of patients stood, 54% walked at least once during their ICU stay, and ICU-acquired pressure ulcers and physical restraint use decreased (period 1 vs 2: 39% vs 23% of patients; 30% vs 26% patient days, respectively; p < 0.001 for both). After adjustment for patient-level covariates, implementation of the full (B-AD-EC) versus partial (B-AD) bundle was associated with reduced mechanical ventilation duration (-22.3%; 95% CI, -22.5% to -22.0%; p < 0.001), ICU length of stay (-10.3%; 95% CI, -15.6% to -4.7%; p = 0.028), and hospital length of stay (-7.8%; 95% CI, -8.7% to -6.9%; p = 0.006). Total ICU and hospital cost were also reduced by 24.2% (95% CI, -41.4% to -2.0%; p = 0.03) and 30.2% (95% CI, -46.1% to -9.5%; p = 0.007), respectively.
Conclusions: In a clinical practice setting, the addition of (E)arly mobilization and structured (C)oordination of ABCDE bundle components to a spontaneous (B)reathing, (A)wakening, and (D) elirium management background led to substantial reductions in the duration of mechanical ventilation, length of stay, and cost.
Figures

Comment in
-
The Awakening and Breathing, Coordination, Delirium Monitoring and Management, and Early Mobilization Bundle (ABCDE): Next Time Won't You Screen With Me.Crit Care Med. 2019 Jul;47(7):997-998. doi: 10.1097/CCM.0000000000003787. Crit Care Med. 2019. PMID: 31205080 No abstract available.
References
-
- Hopkins RO, Weaver LK, Collingridge D, et al.: Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med 2005; 171: 340–347 - PubMed
-
- Puthucheary ZA, Rawal J, McPhail M, et al.: Acute skeletal muscle wasting in critical illness. JAMA 2013; 310: 1591–1600 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
