

Intraductal Oncocytic Papillary Neoplasms: Clinical-Pathologic Characterization of 24 Cases, With An Emphasis on Associated Invasive Carcinomas
- PMID: 30986801
- PMCID: PMC6467507
- DOI: 10.1097/PAS.0000000000001226
Intraductal Oncocytic Papillary Neoplasms: Clinical-Pathologic Characterization of 24 Cases, With An Emphasis on Associated Invasive Carcinomas
Abstract
Background: Intraductal oncocytic papillary neoplasm (IOPN) of the pancreas is a rare tumor. Recent molecular data indicate that it is distinct from other intraductal neoplasms; however, its clinicopathologic characteristics, especially the frequency/significance of an invasive carcinoma component, and biologic behavior remain to be fully defined.
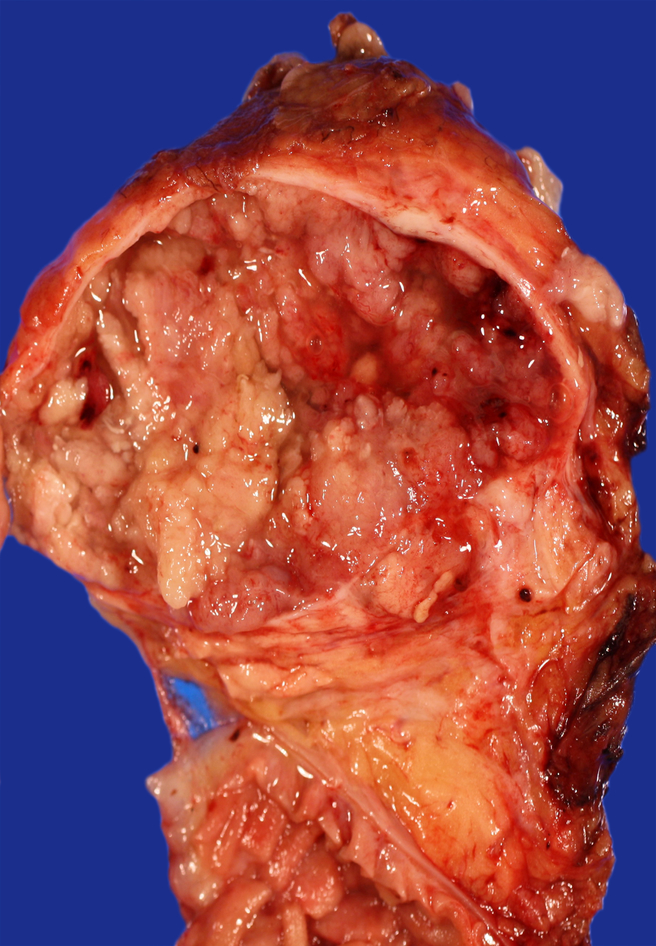
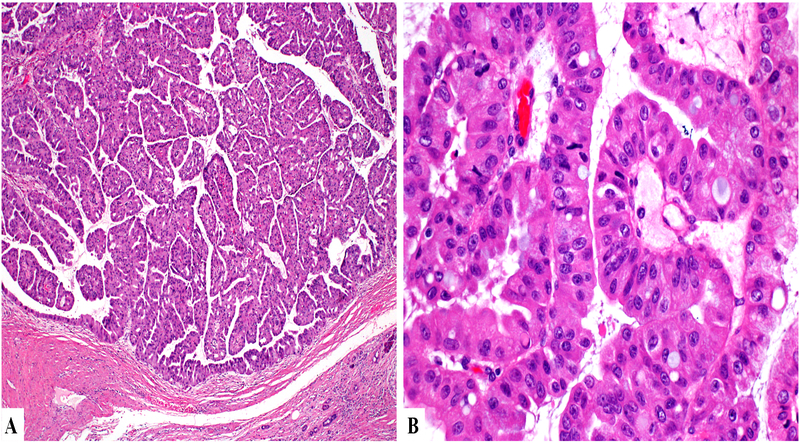
Design: Clinicopathologic characteristics and survival of 24 IOPNs were analyzed. By definition, all tumors exhibited intraductal growth and oncocytic morphology.
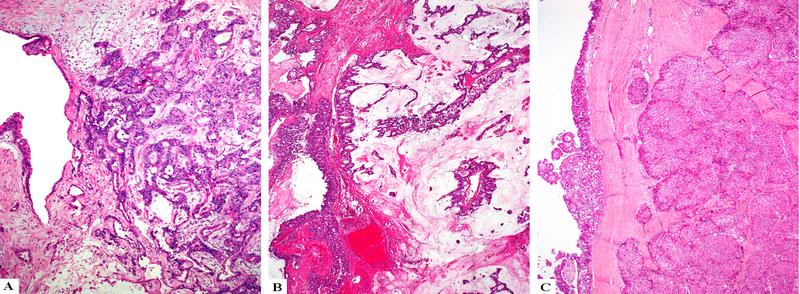
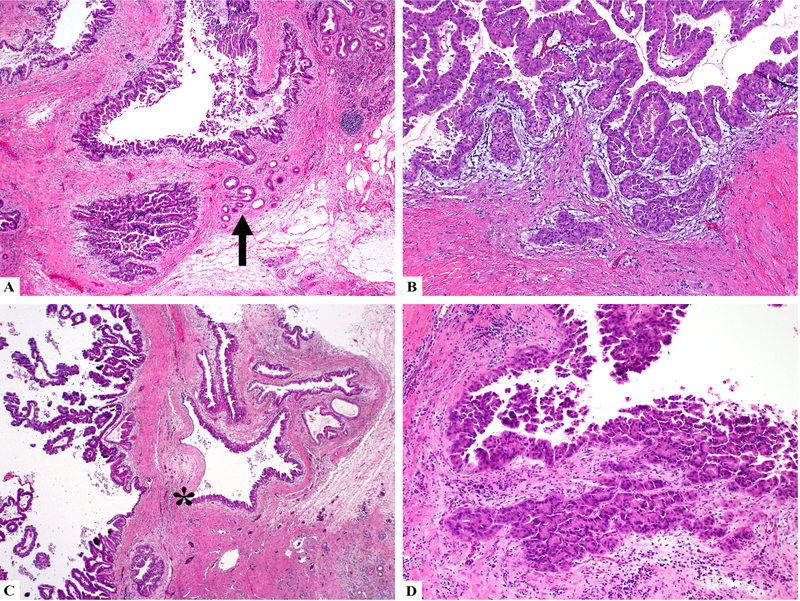
Results: The female:male ratio was 1.7, and mean age was 59. In 44% of the patients, the IOPN was discovered incidentally; however, the working diagnosis was "ductal adenocarcinoma" in 42%. Fourteen IOPNs occurred in the head of the pancreas. The median tumor size was 4.5 cm. The tumors often grew along adjacent benign ducts, mimicking invasion, but only 29% exhibited unequivocal invasive carcinoma, mostly in the form of microscopic foci (pT1a=4, pT1b=1, pT2=2), and only 6% had lymph node metastasis. Invasive carcinoma was predominantly composed of small tubular units lined by oncocytic cells, or individual oncocytic cells infiltrating the periductal stroma. Follow-up information was available for 18 patients (median=6.8 y). No patients died from the disease, and the overall 10-year survival was 94%. Patients with invasive carcinoma trended toward a lower 5-year recurrence-free survival than those with noninvasive IOPNs (66% vs. 93%, P=0.066), but overall survival was not impacted by the presence of invasion (P=0.38).
Conclusions: IOPN is a distinct tumor type in the pancreas. Despite its morphologic complexity and often extensive pagetoid spread to adjacent ducts, conventional invasive carcinoma is seen in only 29% and usually as microscopic foci. Thus, it is not surprising that IOPN exhibits indolent behavior even when invasion is present.
Conflict of interest statement
DISCLOSURE
Supported in part by the Cancer Center Support Grant (CCSG)/Core Grant/P30 CA008748 and by the Melamed Family Foundation. The remaining authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Figures
References
-
- Adsay NV, Adair CF, Heffess CS, et al. Intraductal oncocytic papillary neoplasms of the pancreas. Am J Surg Pathol. 1996;20:980–994. - PubMed
-
- Adsay NV, Kloppel G, Fukushima N, et al. Intraductal neoplasms of the pancreas In: Bosman FT, Carneiro F, Hruban RH, eds. WHO Classification of Tumors. Lyon, France: WHO Press; 2010:pp 304–313.
-
- Adsay NV. Cystic lesions of the pancreas. Mod Pathol. 2007;20 Suppl 1:S71–93. - PubMed
-
- Basturk O, Khayyata S, Klimstra DS, et al. Preferential expression of MUC6 in oncocytic and pancreatobiliary types of intraductal papillary neoplasms highlights a pyloropancreatic pathway, distinct from the intestinal pathway, in pancreatic carcinogenesis. Am J Surg Pathol. 2010;34:364–370. - PMC - PubMed
-
- Kloppel G, Basturk O, Schlitter AM, et al. Intraductal neoplasms of the pancreas. Semin Diagn Pathol. 2014;31:452–466. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
