

Epinephrine in Neonatal Resuscitation
- PMID: 30987062
- PMCID: PMC6518253
- DOI: 10.3390/children6040051
Epinephrine in Neonatal Resuscitation
Abstract
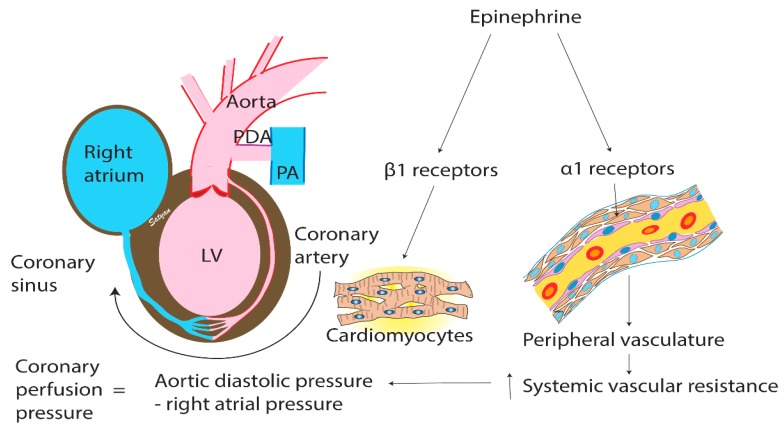
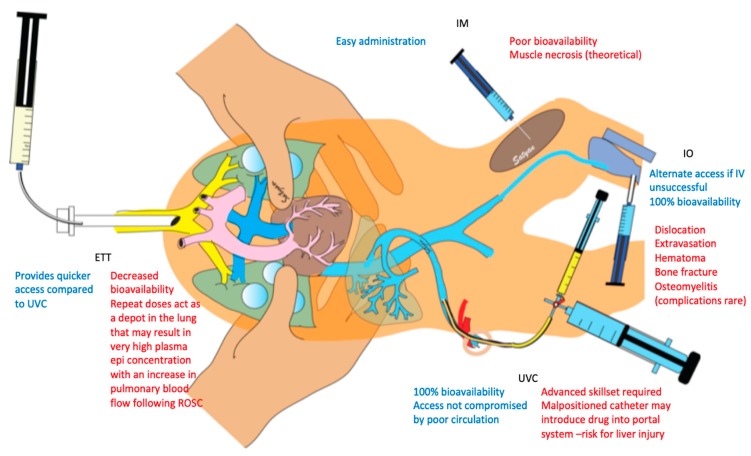
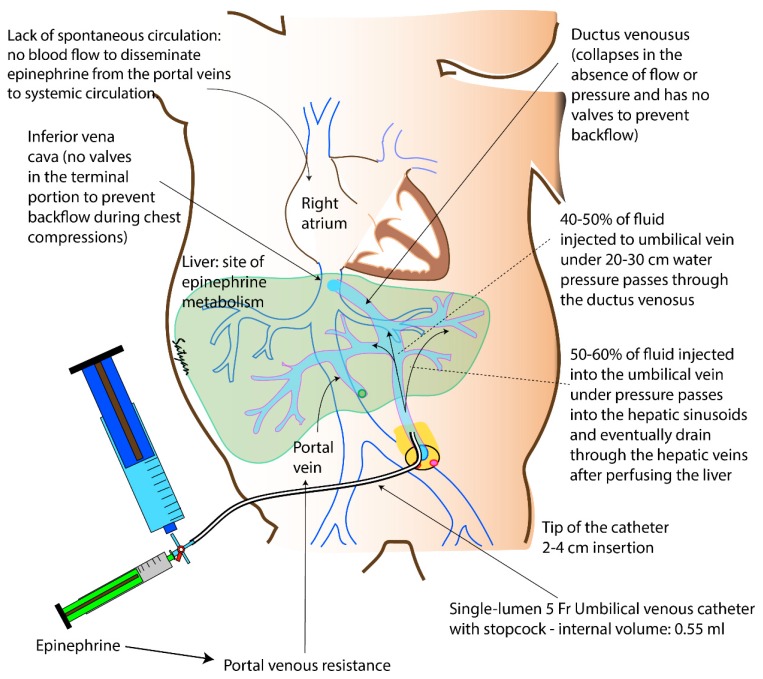
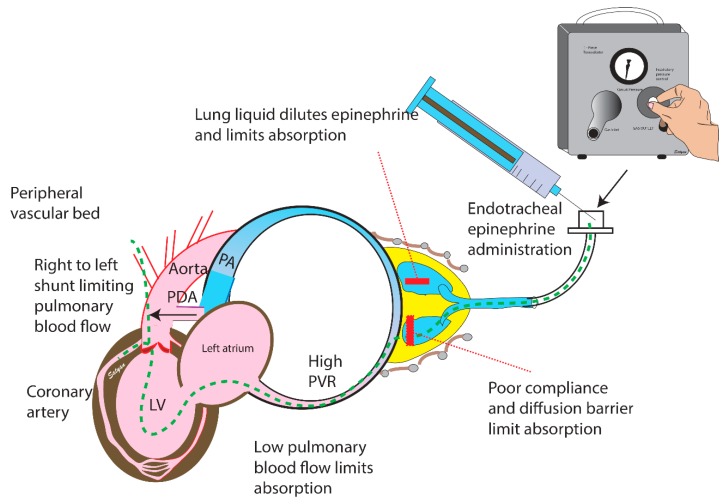
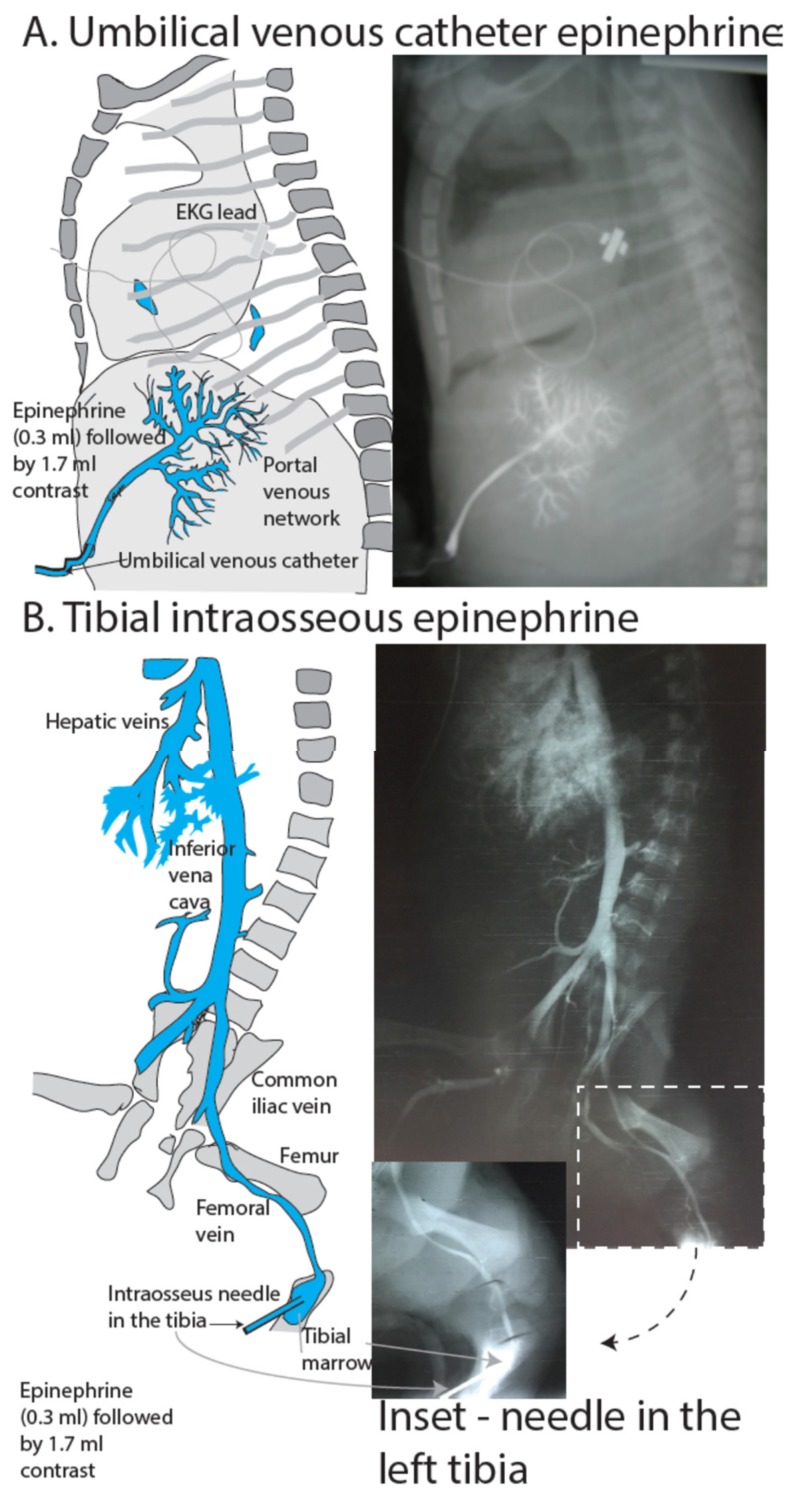
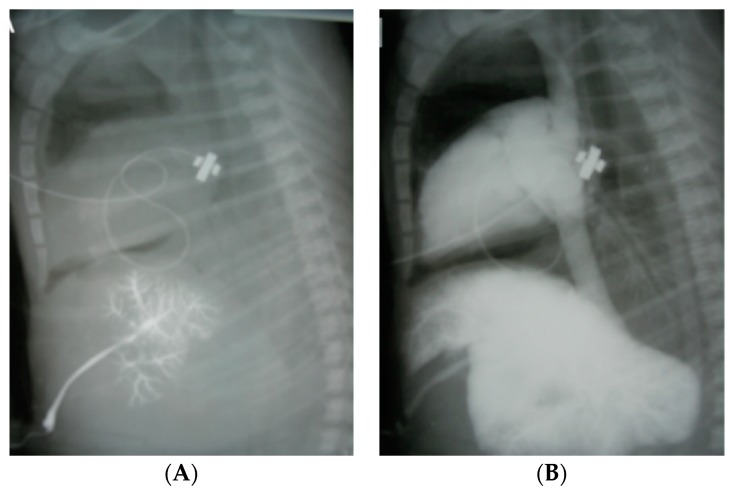
Epinephrine is the only medication recommended by the International Liaison Committee on Resuscitation for use in newborn resuscitation. Strong evidence from large clinical trials is lacking owing to the infrequent use of epinephrine during neonatal resuscitation. Current recommendations are weak as they are extrapolated from animal models or pediatric and adult studies that do not adequately depict the transitioning circulation and fluid-filled lungs of the newborn in the delivery room. Many gaps in knowledge including the optimal dosing, best route and timing of epinephrine administration warrant further studies. Experiments on a well-established ovine model of perinatal asphyxial cardiac arrest closely mimicking the newborn infant provide important information that can guide future clinical trials.
Keywords: epinephrine; intramuscular; intraosseous; intravenous; newborn; resuscitation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cardiac Agents during Neonatal Cardiopulmonary Resuscitation.Neonatology. 2024;121(2):157-166. doi: 10.1159/000535502. Epub 2024 Jan 16. Neonatology. 2024. PMID: 38228124 Review.
-
The International Liaison Committee on Resuscitation (ILCOR) consensus on science with treatment recommendations for pediatric and neonatal patients: pediatric basic and advanced life support.Pediatrics. 2006 May;117(5):e955-77. doi: 10.1542/peds.2006-0206. Epub 2006 Apr 17. Pediatrics. 2006. PMID: 16618790
-
2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support.Pediatrics. 2006 May;117(5):e989-1004. doi: 10.1542/peds.2006-0219. Pediatrics. 2006. PMID: 16651298
-
Epinephrine Use during Newborn Resuscitation.Front Pediatr. 2017 May 1;5:97. doi: 10.3389/fped.2017.00097. eCollection 2017. Front Pediatr. 2017. PMID: 28507983 Free PMC article. Review.
-
Drug routes in out-of-hospital cardiac arrest: A summary of current evidence.Resuscitation. 2022 Dec;181:70-78. doi: 10.1016/j.resuscitation.2022.10.015. Epub 2022 Oct 26. Resuscitation. 2022. PMID: 36309248 Review.
Cited by
-
Optimal oxygen use in neonatal advanced cardiopulmonary resuscitation-a literature review.Pediatr Med. 2023 May 30;6:16. doi: 10.21037/pm-21-74. Epub 2022 Feb 21. Pediatr Med. 2023. PMID: 39364342 Free PMC article.
-
Singapore Neonatal Resuscitation Guidelines 2021.Singapore Med J. 2021 Aug;62(8):404-414. doi: 10.11622/smedj.2021110. Singapore Med J. 2021. PMID: 35001116 Free PMC article.
-
Vasopressin versus epinephrine during cardiopulmonary resuscitation of asphyxiated newborns: A study protocol for a prospective, cluster, open label, single-center, randomized controlled phase 2 trial - The VERSE-Trial.Resusc Plus. 2023 Aug 31;16:100459. doi: 10.1016/j.resplu.2023.100459. eCollection 2023 Dec. Resusc Plus. 2023. PMID: 37663146 Free PMC article.
-
Effect of a Larger Flush Volume on Bioavailability and Efficacy of Umbilical Venous Epinephrine during Neonatal Resuscitation in Ovine Asphyxial Arrest.Children (Basel). 2021 Jun 1;8(6):464. doi: 10.3390/children8060464. Children (Basel). 2021. PMID: 34205843 Free PMC article.
-
What is the optimal initial dose of epinephrine during neonatal resuscitation in the delivery room?J Perinatol. 2021 Jul;41(7):1769-1773. doi: 10.1038/s41372-021-01032-7. Epub 2021 Mar 12. J Perinatol. 2021. PMID: 33712718 Free PMC article. Review.
