

Cardiovascular determinants of resuscitation from sepsis and septic shock
- PMID: 30987647
- PMCID: PMC6466803
- DOI: 10.1186/s13054-019-2414-9
Cardiovascular determinants of resuscitation from sepsis and septic shock
Abstract
Background: We hypothesized that the cardiovascular responses to Surviving Sepsis Guidelines (SSG)-defined resuscitation are predictable based on the cardiovascular state.
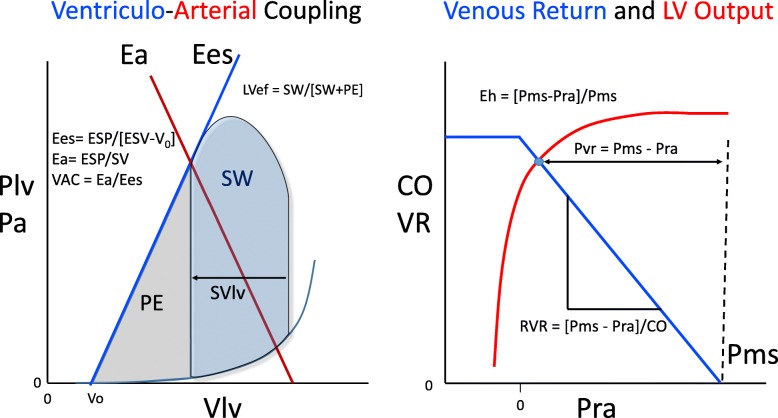
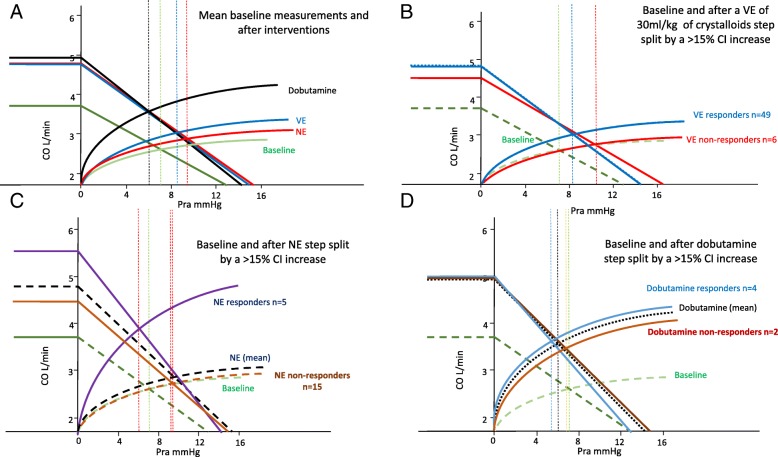
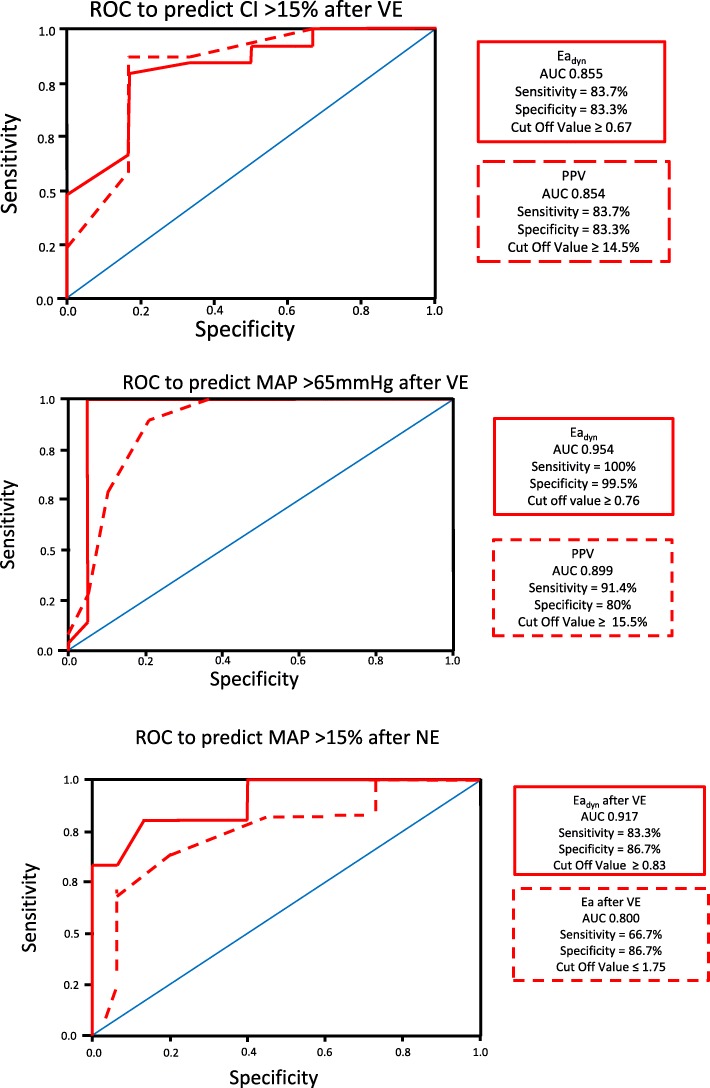
Methods: Fifty-five septic patients treated by SSG were studied before and after volume expansion (VE), and if needed norepinephrine (NE) and dobutamine. We measured mean arterial pressure (MAP), cardiac index (CI), and right atrial pressure (Pra) and calculated pulse pressure and stroke volume variation (PPV and SVV), dynamic arterial elastance (Eadyn), arterial elastance (Ea) and left ventricular (LV) end-systolic elastance (Ees), Ees/Ea (VAC), LV ejection efficiency (LVeff), mean systemic pressure analogue (Pmsa), venous return pressure gradient (Pvr), and cardiac performance (Eh), using standard formulae.
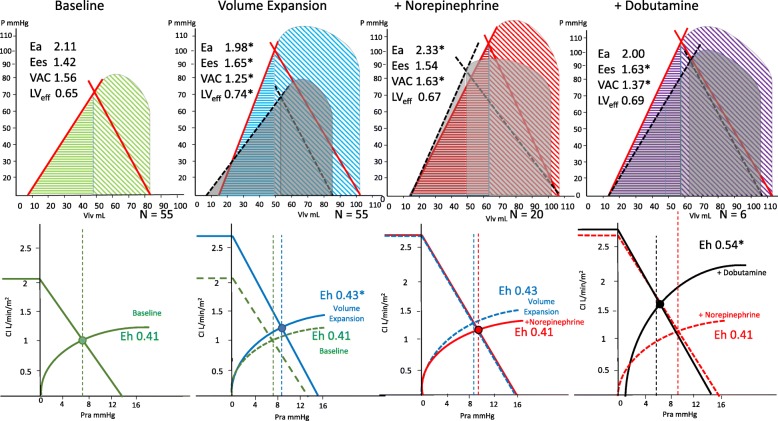
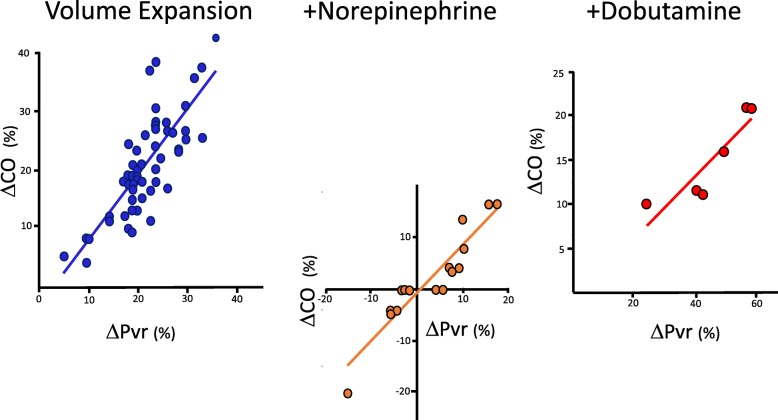
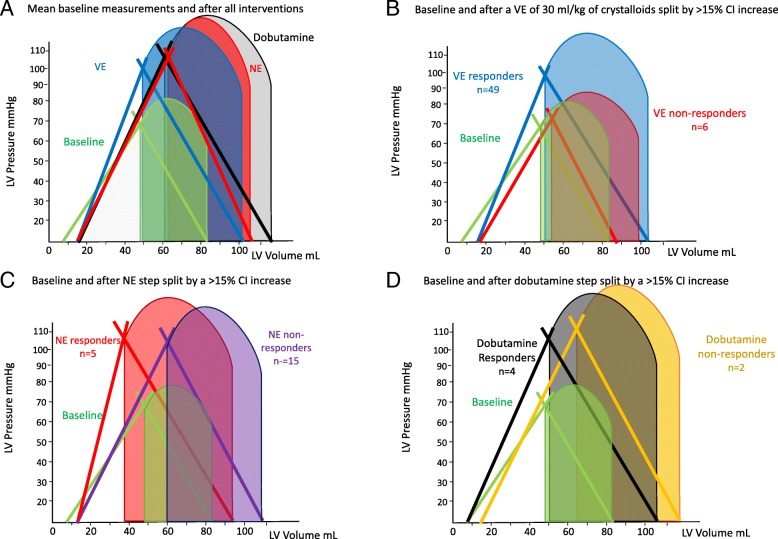
Results: All patients were hypotensive (MAP 56.8 ± 3.1 mmHg) and tachycardic (113.1 ± 7.5 beat min-1), with increased lactate levels (lactate = 5.0 ± 4.2 mmol L-1) with a worsened VAC. CI was variable but > 2 L min-1 M-2 in 74%. Twenty-eight-day mortality was 48% and associated with admission lactate, blood urea nitrogen (BUN), and creatinine levels but not cardiovascular state. In all patients, both MAP and CI improved following VE, as well as cardiac contractility (Ees). Fluid administration improved Pra, Pmsa, and Pvr in all patients, whereas both HR and Ea decreased after VE, thus normalizing VAC. CI increases were proportional to baseline PPV and SVV. CI increases proportionally decreased PPV and SVV. VE increased MAP > 65 mmHg in 35/55 patients. MAP responders had higher PPV, SVV, and Eadyn than non-responders. NE was given to 20/55 patients in septic shock, but increased MAP > 65 mmHg in only 12. NE increased Ea, Eadyn, Pra, Pmsa, and VAC while decreasing HR, PPV, SVV, and LVeff. MAP responders had higher pre-NE Ees and lower VAC. Dobutamine was given to 6/8 patients who remained hypotensive following NE. It increased Ees, MAP, CI, and LVeff, while decreasing HR, Pra, and VAC. At all times and all steps of the protocol, CI changes were proportional to Pvr changes independent of treatment.
Conclusions: The cardiovascular response to SSG-based resuscitation is highly heterogeneous but predictable from pre-treatment measures of cardiovascular state.
Keywords: Blood volume; Clinical trial; Effective circulating blood volume; Heart-lung interactions; Norepinephrine; Ventriculo-arterial coupling.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by both institutions’ review boards for human experimentation. All subjects who regained consciousness signed informed consent while those who did not did not sign but by Italian law were permitted to be included in this study.
Consent for publication
The authors agree to waive copyright and allow this manuscript to be published in Critical Care.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche J-D, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2006;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
