

Comparative Performance of Urinary Biomarkers for Vancomycin-Induced Kidney Injury According to Timeline of Injury
- PMID: 30988153
- PMCID: PMC6591602
- DOI: 10.1128/AAC.00079-19
Comparative Performance of Urinary Biomarkers for Vancomycin-Induced Kidney Injury According to Timeline of Injury
Abstract
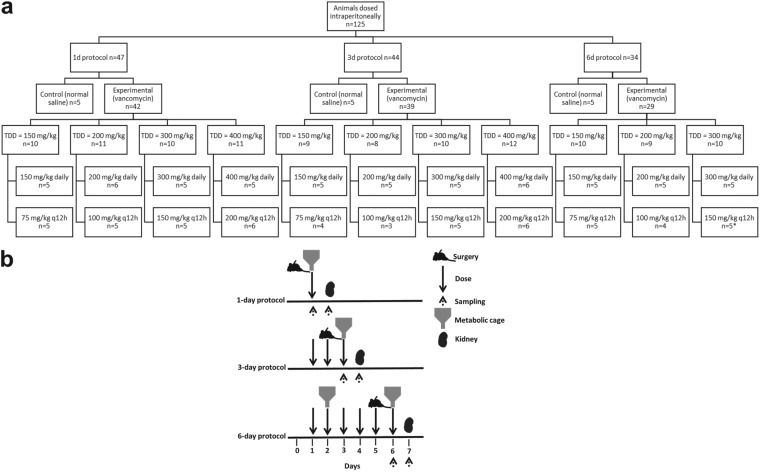
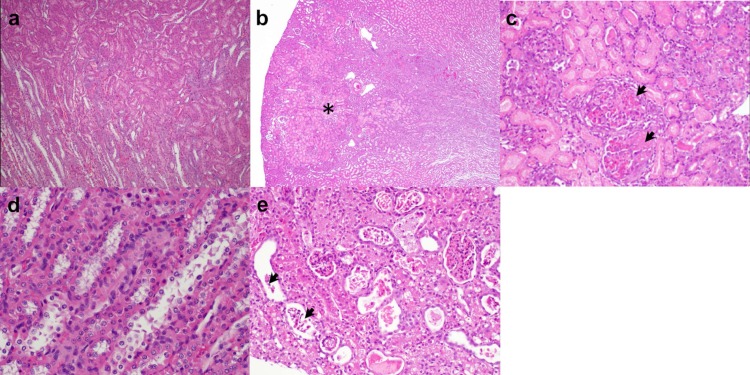
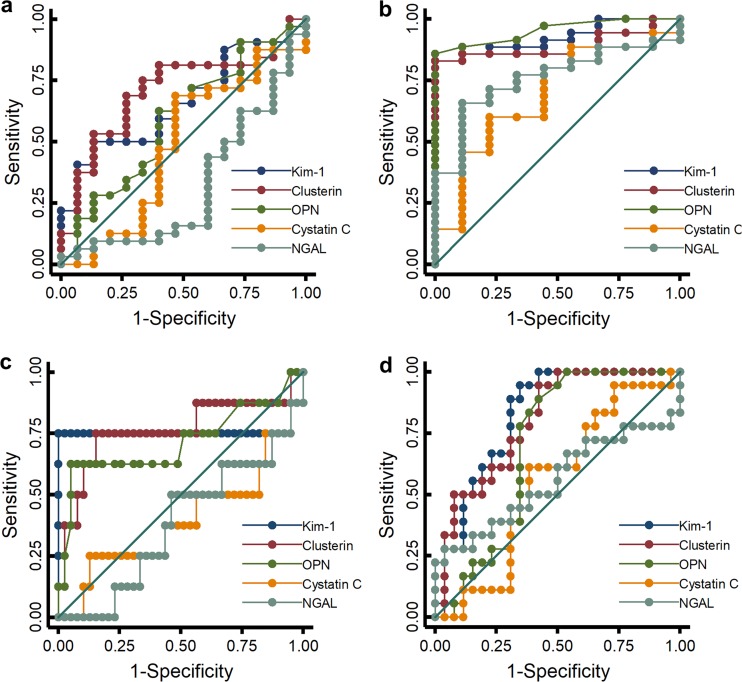
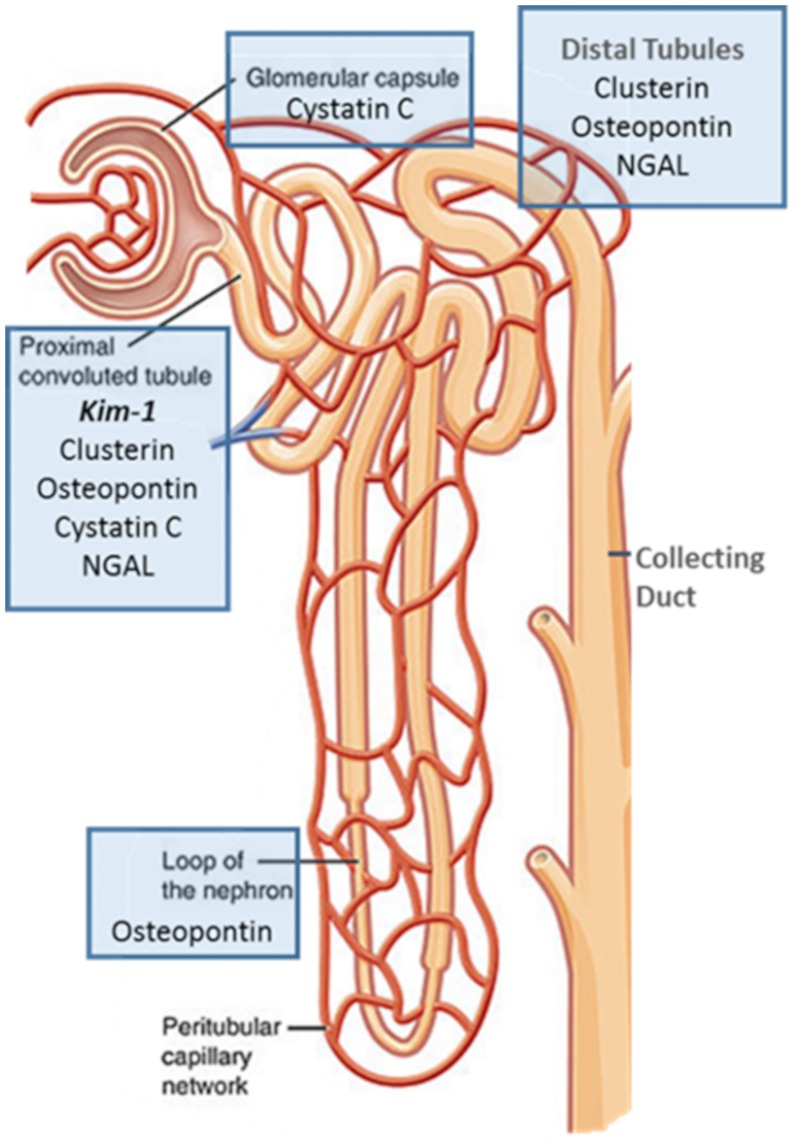
Urinary biomarkers are superior to serum creatinine for defining onset and extent of kidney injury. This study classifies the temporal predictive ability of biomarkers for vancomycin-induced kidney injury (VIKI) as defined by histopathologic damage. Male Sprague-Dawley rats (n = 125) were randomized to receive 150 to 400 mg/kg of body weight/day vancomycin via once or twice daily intraperitoneal injection over 1, 3, or 6 days. Urine was collected once during the 24 h prior to euthanasia or twice for rats treated for 6 days. Receiver operating characteristic (ROC) curves were employed to assess the urinary biomarker performances of kidney injury molecule 1 (KIM-1), clusterin, osteopontin (OPN), cystatin C, and neutrophil gelatinase-associated lipocalin (NGAL) to predict histopathologically defined VIKI (using a national standard pathological assessment scheme from hematoxylin and eosin stained kidneys). Urinary KIM-1, clusterin, and OPN outperformed cystatin C and NGAL with regard to sensitivity and specificity. For the earliest injury, urinary KIM-1 (area under the receiver operating characteristic curve [AUC], 0.662; P < 0.001) and clusterin (AUC, 0.706; P < 0.001) were the most sensitive for predicting even low-level histopathologic damage at 24 h compared to NGAL. KIM-1 and clusterin are the earliest and most sensitive predictors of VIKI. As injury progresses, KIM-1, clusterin, and OPN best define the extent of damage.
Keywords: KIM-1; PK/PD; PK/TD; biomarker; histopathology; injury; kidney; toxicity; urinary; vancomycin.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Kelesidis T, Braykov N, Uslan DZ, Morgan DJ, Gandra S, Johannsson B, Schweizer ML, Weisenberg SA, Young H, Cantey J, Perencevich E, Septimus E, Srinivasan A, Laxminarayan R. 2016. Indications and types of antibiotic agents used in 6 acute care hospitals, 2009–2010: a pragmatic retrospective observational study. Infect Control Hosp Epidemiol 37:70–79. doi: 10.1017/ice.2015.226. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
