

A population pharmacokinetic study of benzathine benzylpenicillin G administration in children and adolescents with rheumatic heart disease: new insights for improved secondary prophylaxis strategies
- PMID: 30989171
- PMCID: PMC6587412
- DOI: 10.1093/jac/dkz076
A population pharmacokinetic study of benzathine benzylpenicillin G administration in children and adolescents with rheumatic heart disease: new insights for improved secondary prophylaxis strategies
Abstract
Background: Benzathine benzylpenicillin G (BPG) is recommended as secondary prophylaxis to prevent recurrence of acute rheumatic fever and subsequent rheumatic heart disease (RHD). Following intramuscular injection, BPG is hydrolysed to benzylpenicillin. Little is known of the pharmacokinetics of benzylpenicillin following BPG in populations at risk of RHD.
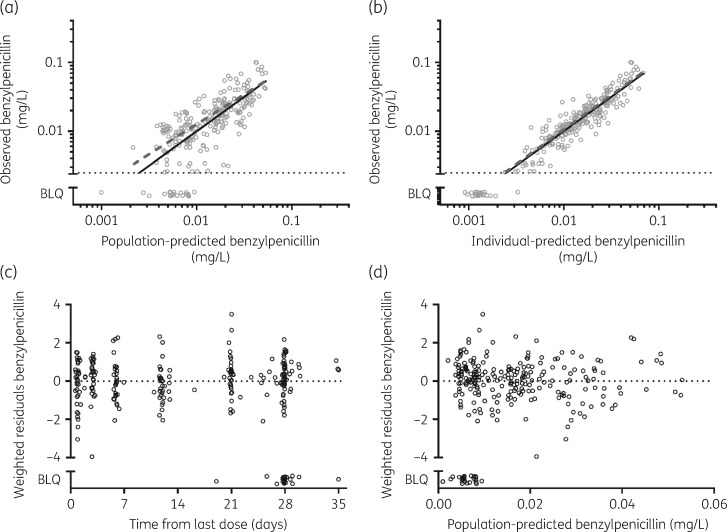
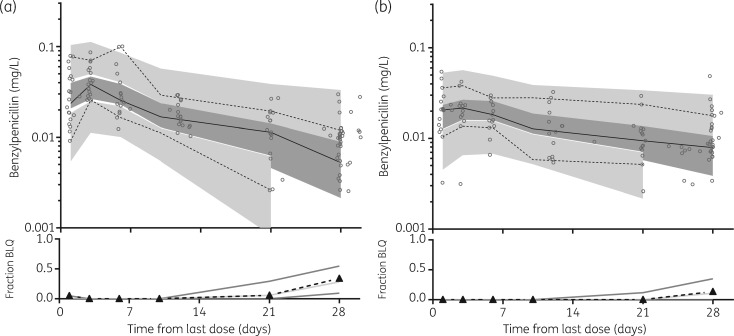
Methods: We conducted a longitudinal pharmacokinetic study of children and adolescents receiving secondary prophylaxis throughout six monthly cycles of BPG. Dried blood spot samples were assayed with LC-MS/MS. Benzylpenicillin concentrations were analysed using non-linear mixed-effects modelling with subsequent simulations based on published BMI-for-age and weight-for-age data.
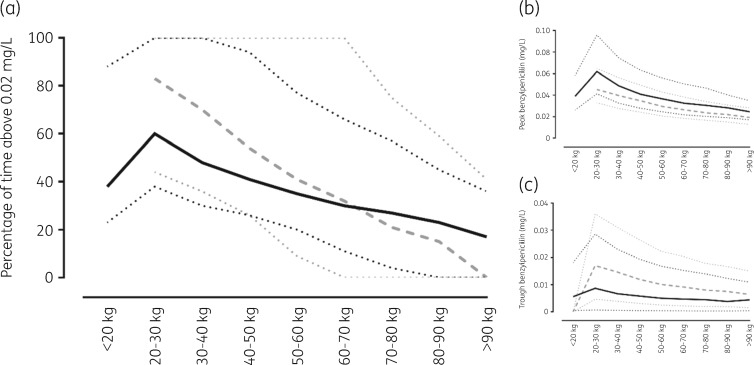
Results: Eighteen participants contributed 256 concentrations for analysis. None had benzylpenicillin concentrations >0.02 mg/L for the full time between doses. The median duration above this target was 9.8 days for those with a lower BMI (<25 kg/m2), who also had lower weights, and 0 days for those with a higher BMI (≥25 kg/m2). Although fat-free mass was a key determinant of benzylpenicillin exposure after a standard dose of BPG, having a higher BMI influenced absorption and almost doubled (increase of 86%) the observed t½.
Conclusions: Few children and adolescents receiving BPG as secondary prophylaxis will achieve concentrations >0.02 mg/L for the majority of the time between injections. The discordance of this observation with reported efficacy of BPG to prevent rheumatic fever implies a major knowledge gap relating to pharmacokinetic/pharmacodynamic relationships between benzylpenicillin exposure and clinical outcomes.
© The Author(s) 2019. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures

References
-
- Carapetis JR, McDonald M, Wilson NJ.. Acute rheumatic fever. Lancet 2005; 366: 155–68. - PubMed
-
- Parks T, Smeesters PR, Steer AC.. Streptococcal skin infection and rheumatic heart disease. Curr Opin Infect Dis 2012; 25: 145–53. - PubMed
-
- O'Sullivan L, Moreland NJ, Webb RH. et al. Acute rheumatic fever after Group A Streptococcus pyoderma and Group G Streptococcus pharyngitis. Pediatr Infect Dis J 2017; 36: 692–4. - PubMed
-
- Watkins DA, Johnson CO, Colquhoun SM. et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med 2017; 377: 713–22. - PubMed
-
- Roberts KV, Maguire GP, Brown A. et al. Rheumatic heart disease in Indigenous children in northern Australia: differences in prevalence and the challenges of screening. Med J Aust 2015; 203: 221.e1–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
