

Progression Risk Stratification of Asymptomatic Waldenström Macroglobulinemia
- PMID: 30990729
- PMCID: PMC6544461
- DOI: 10.1200/JCO.19.00394
Progression Risk Stratification of Asymptomatic Waldenström Macroglobulinemia
Abstract
Background: Waldenström macroglobulinemia (WM) is preceded by asymptomatic WM (AWM), for which the risk of progression to overt disease is not well defined.
Methods: We studied 439 patients with AWM, who were diagnosed and observed at Dana-Farber Cancer Institute between 1992 and 2014.
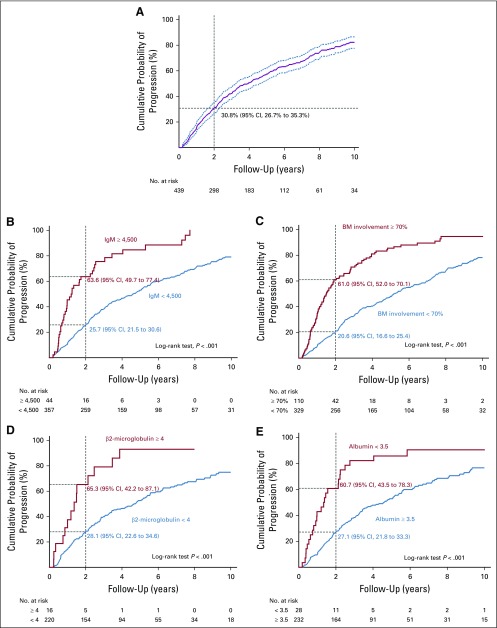
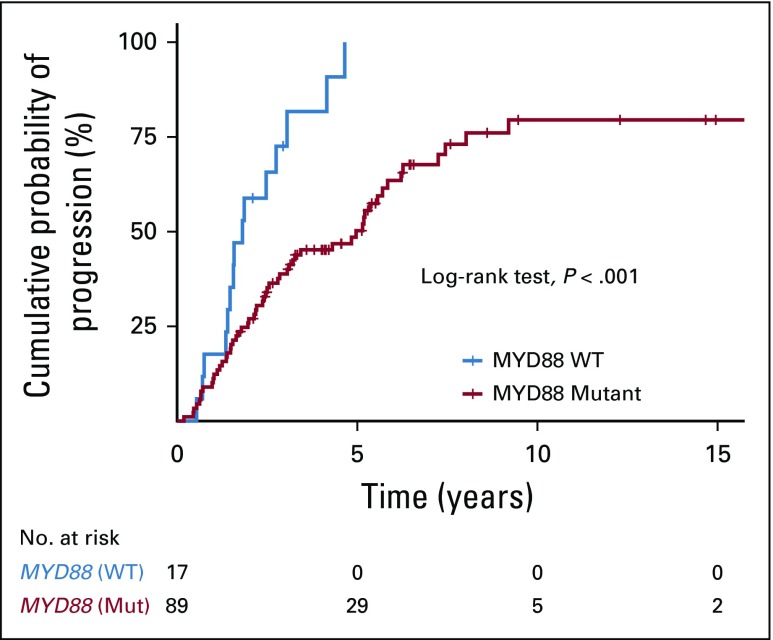
Results: During the 23-year study period, with a median follow-up of 7.8 years, 317 patients progressed to symptomatic WM (72%). Immunoglobulin M 4,500 mg/dL or greater, bone marrow lymphoplasmacytic infiltration 70% or greater, β2-microglobulin 4.0 mg/dL or greater, and albumin 3.5 g/dL or less were all identified as independent predictors of disease progression. To assess progression risk in patients with AWM, we trained and cross-validated a proportional hazards model using bone marrow infiltration, immunoglobulin M, albumin, and beta-2 microglobulin values as continuous measures. The model divided the cohort into three distinct risk groups: a high-risk group with a median time to progression (TTP) of 1.8 years, an intermediate-risk group with a median TTP of 4.8 years, and a low-risk group with a median TTP of 9.3 years. We validated this model in two external cohorts, demonstrating robustness and generalizability. For clinical applicability, we made the model available as a Web page application ( www.awmrisk.com ). By combining two cohorts, we were powered to identify wild type MYD88 as an independent predictor of progression (hazard ratio, 2.7).
Conclusion: This classification system is positioned to inform patient monitoring and care and, for the first time to our knowledge, to identify patients with high-risk AWM who may need closer follow-up or benefit from early intervention.
Figures

Comment in
-
Asymptomatic Waldenström Macroglobulinemia: Should We Consider a Different Terminology?J Clin Oncol. 2019 Oct 10;37(29):2700-2701. doi: 10.1200/JCO.19.01392. Epub 2019 Aug 19. J Clin Oncol. 2019. PMID: 31424979 No abstract available.
-
Reply to F.D. Leonard.J Clin Oncol. 2019 Oct 10;37(29):2701-2702. doi: 10.1200/JCO.19.01708. Epub 2019 Aug 19. J Clin Oncol. 2019. PMID: 31424980 No abstract available.
References
-
- Castillo JJ, Ghobrial IM, Treon SP. Biology, prognosis, and therapy of Waldenström Macroglobulinemia. Cancer Treat Res. 2015;165:177–195. - PubMed
-
- Owen RG, Treon SP, Al-Katib A, et al. Clinicopathological definition of Waldenstrom’s macroglobulinemia: Consensus panel recommendations from the Second International Workshop on Waldenstrom’s Macroglobulinemia. Semin Oncol. 2003;30:110–115. - PubMed
-
- Gertz MA. Waldenström macroglobulinemia: 2017 update on diagnosis, risk stratification, and management. Am J Hematol. 2017;92:209–217. - PubMed
-
- Wang H, Chen Y, Li F, et al. Temporal and geographic variations of Waldenstrom macroglobulinemia incidence: A large population-based study. Cancer. 2012;118:3793–3800. - PubMed
-
- Kastritis E, Leblond V, Dimopoulos MA, et al: Waldenstrom’s macroglobulinaemia: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 24:vi155-vi159, 2018. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
